Third-trimester scan
Third-trimester scan guidelines
These guidelines were published in 2019 and are awaiting review, due 2022. Some content may be outdated.
Note: A growth scan is not recommended in women where symphysial-fundal height (SFH) is tracking along or above the 90th centile if gestational diabetes has been excluded and there is no clinical concern regarding polyhydramnios (see the SGA guideline (PDF, 2.9 MB) for more detail, NZMFMN 2014a).
[1] See Appendix 1: Ultrasound scan codes and indications.
Note: In the absence of any clinical indications, routine post-date scanning is not currently recommended.
Growth charts as per local protocol. At present, ASUM are used in most sites.
As per the SGA guideline (PDF, 2.9 MB) and Obstetric Doppler guideline (PDF, 3.7 MB) (NZMFMN 2014a and 2014b respectively), suboptimal fetal growth is suspected when:
The minimum interval between growth scans is 14 days. See Appendix 9: SGA scanning schedule.
Routine Doppler is not indicated.
For more detail, see the SGA guideline (PDF, 2.9 MB) and Obstetric Doppler guideline (PDF, 3.7 MB) (NZMFMN 2014a and 2014b respectively) for Doppler indications and the Doppler chapter.
This assessment is for uncomplicated scans performed after 20 weeks, assuming a previous normal anatomy scan.
For otherwise uncomplicated serial scans, detailed assessment of anatomy is only necessary once in the third trimester.
For the first scan in the third trimester, image:
If growth assessment as above has been performed within the last two weeks, a limited fluid and Doppler scan may be indicated, particularly as directed by the SGA pathway (see Appendix 9).
Routine assessment as per Third-trimester ultrasound examination above, with additional views as below.
The recommended frequency of scans for women with gestational diabetes is outlined in Screening, Diagnosis and Management of Gestational Diabetes in New Zealand: A clinical practice guideline (Ministry of Health 2014).
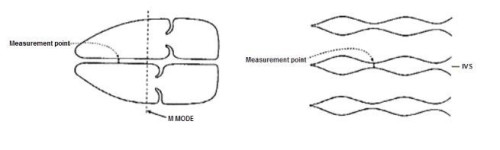
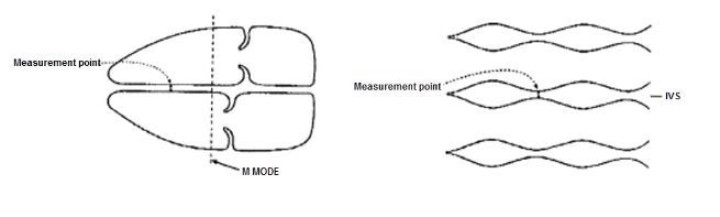
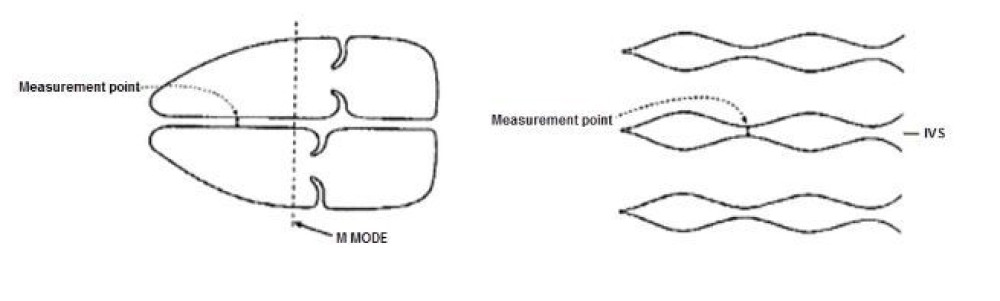
An increase in fetal IVS and ventricular wall thickness is reported in diabetic pregnancy. These babies are at increased risk of cardiomyopathy. Consider measurement of the IVS in diabetic patients with EFW ≥90th centile.
Source: Canterbury DHB Obstetric and Gynaecology Ultrasound Protocols, June 2019 (internal DHB document).
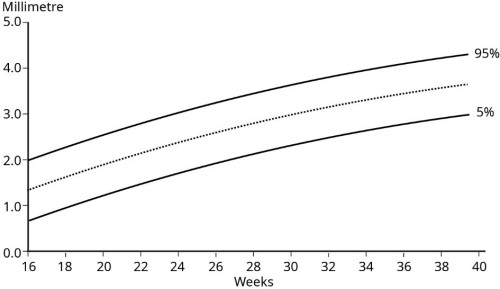
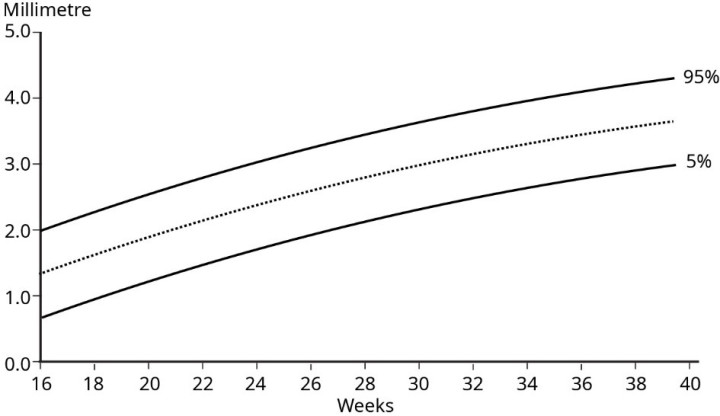
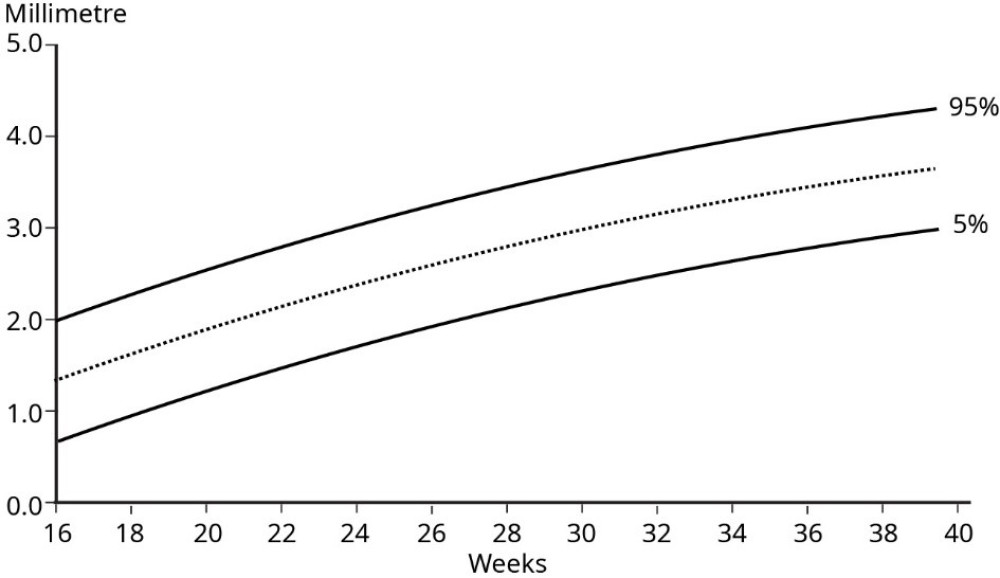
Source: Tan et al 1992.
See Twin pregnancy chapter and the guideline Multiple Pregnancy (PDF, 318 KB) (NZMFMN 2015f).
Assess relevant anatomy, for example, fetal renal tract – see Appendix 7: Fetal renal tract dilation charts.
See the SGA guideline (PDF, 2.9 MB) (NZMFMN 2014a) and Appendix 9: SGA scanning schedule.
Emergency
Urgent
Same day