Placenta
Placenta scan guidelines
These guidelines were published in 2019 and are awaiting review, due 2022. Some content may be outdated.
The placenta is inserted wholly or partially into the lower segment of the uterus. Terms used to describe types of placenta previa include:

Complete placenta previa.
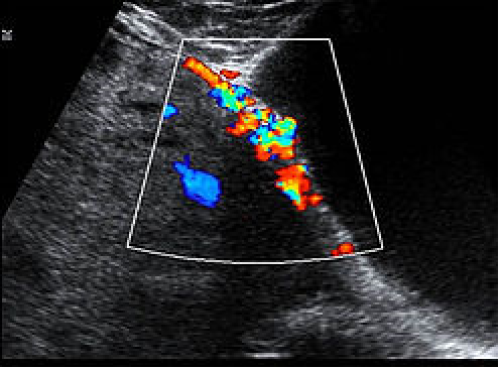
Vasa previa occurs when exposed fetal vessels within the amniotic membranes cover, or are within 20 mm of, the internal cervical os.
This is a clinically significant condition as the vessels are from the fetoplacental circulation, and rupture will lead to rapid fetal exsanguination and death.
There are two types of vasa previa.
Type I vasa previa, with a velamentous cord insertion and vessels coursing over the internal os.
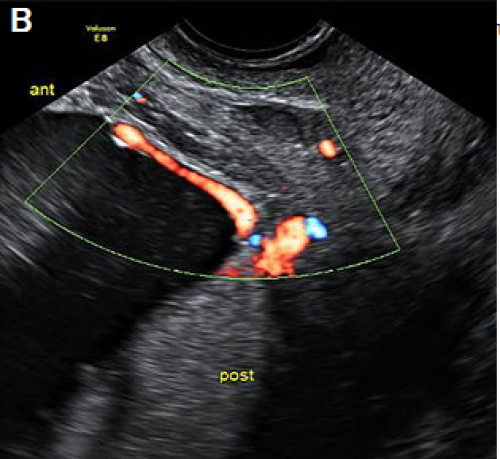
Type II vasa previa, with vessels coursing over the cervix between the main posterior placental lobe and a smaller anterior succenturiate lobe.
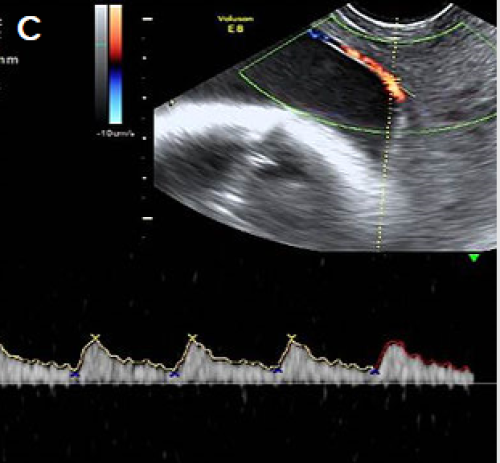
Pulsed Doppler showing a fetal arterial waveform in the vessels crossing the cervix.
For more detail, see The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) statement Vasa Praevia (PDF, 9.1 MB) (RANZCOG 2016).
If a low-lying placenta and/or placenta previa (see above) is found at the anatomy scan, recommend follow-up at approximately 32 weeks gestation, which may include a TV scan.
If there is evidence of vasa previa (see above) at the anatomy scan, report the finding and recommend specialist review and follow-up scans.
Placenta accreta / abnormally invasive placenta (AIP) is a disorder of placental implantation where there is invasion of placental tissue into the uterine wall. It is associated with a high risk of maternal and fetal morbidity and mortality.
Careful assessment is recommended with women who have had a previous caesarean section where the placenta overlies the scar, and if there are any concerns, tertiary opinion is recommended.
Traditionally, the extent may be mild, moderate or severe. However, this can be difficult to assess accurately on ultrasound.
The most common risk factors are a previous caesarean section and placenta previa (see above).
Features of abnormal placental implantation include:
For first-trimester features, see Appendix 2: Low gestational sac in the first trimester with previous caesarean section.
For more detail, see:
If there are features suspicious for placenta accreta at the anatomy scan, recommend specialist referral and follow-up detailed scan.

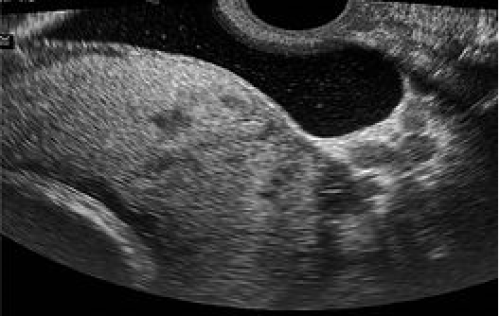
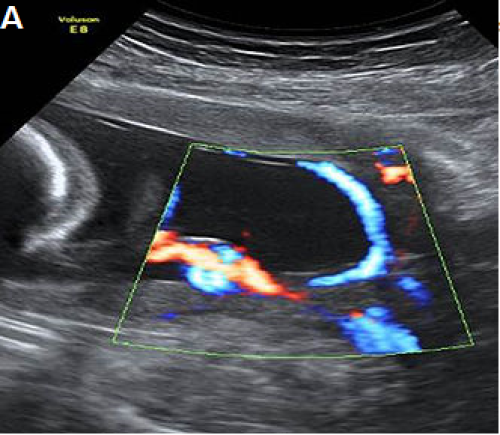
Lower uterine segment and partially filled bladder TV with power Doppler
Complete placenta previa
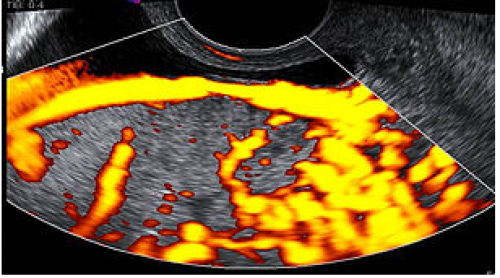
Loss of clear zone
Marked placental bed hypervascularity
Placental lacunae and feeder vessels
Highly suspicious for placenta accreta on colour Doppler imaging.
Emergency