Doppler
Information on Doppler guidelines
These guidelines were published in 2019 and are awaiting review, due 2022. Some content may be outdated.
Doppler assessment should follow the national guidelines recommended in the SGA (PDF, 2.9 MB) and Obstetric Doppler guidelines (PDF, 3.7 MB) (NZMFMN 2014a and 2014b respectively).
Routine fetal Doppler is not indicated in a normal, low-risk pregnancy.
For more detail, see Doppler in Obstetrics (PDF, 16.2 MB) (Nicolaides et al 2002).
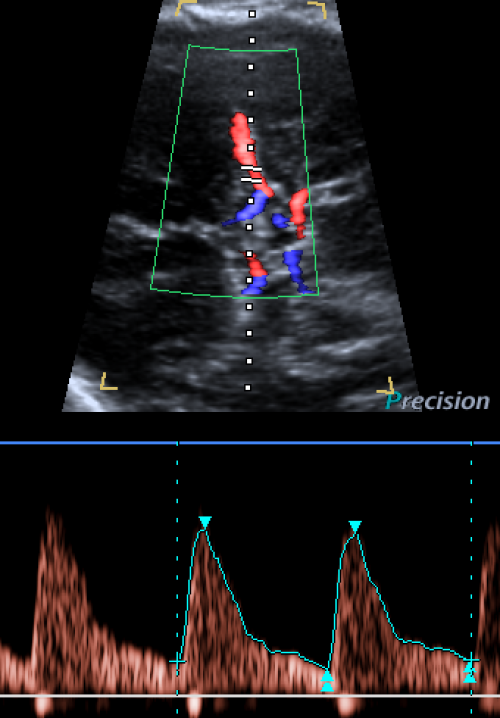
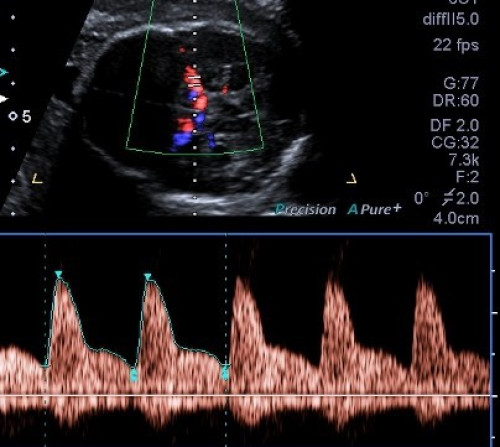
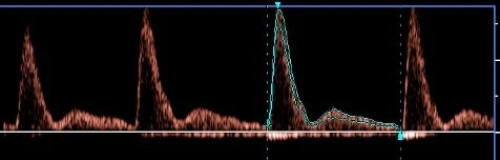
The abnormal UA waveform shows progressive high-resistance flow with reduced, absent and then reversed diastolic flow.
>95th percentile is abnormal.
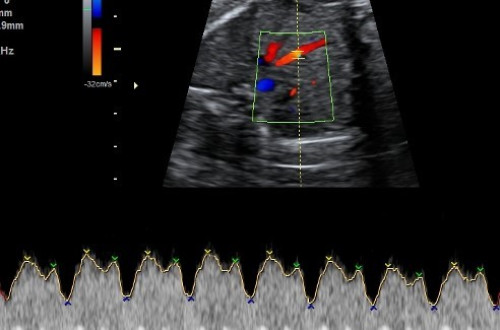
Abnormal MCA PI indicates fetal compensation by redistribution of fetal blood flow to the brain (‘brain sparing’) and shows progressive low-resistance flow with increasing diastolic flow.
<5th percentile is abnormal.
If MCA PI assessment is performed, the CPR should be calculated and recorded.
The CPR is the ratio of MCA PI and UA PI (ie, MCA PI divided by UA PI).
<5th percentile is abnormal.
DV can be technically challenging to measure and should only be performed by experienced individuals.
An abnormal DV PI (± absent or reversed atrial (A) wave) indicates fetal cardiac decompensation.
>95th percentile is abnormal.
Abnormal mean uterine artery pulsatility index
>1.5 MoM is abnormal.
See New Zealand Obstetric Doppler Guideline (PDF, 16.2 MB) [PDF, 3.7 MB] (NZMFMN 2014b).
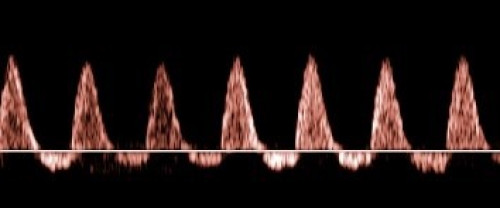
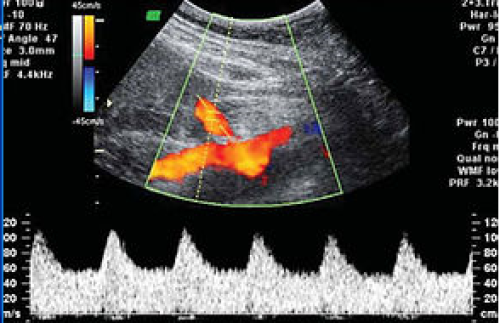
Normal umbilical artery Doppler: Low resistance.
Abnormal: High PI / resistive index (high resistance trace).
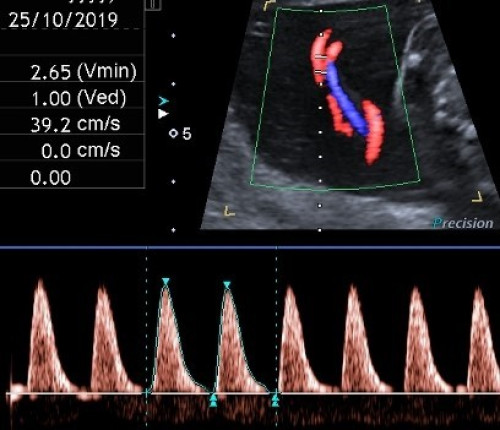
Abnormal: Very high PI / resistive index with absent end-diastolic flow and pulsatility in the umbilical vein.
Abnormal: Reversed end-diastolic flow.
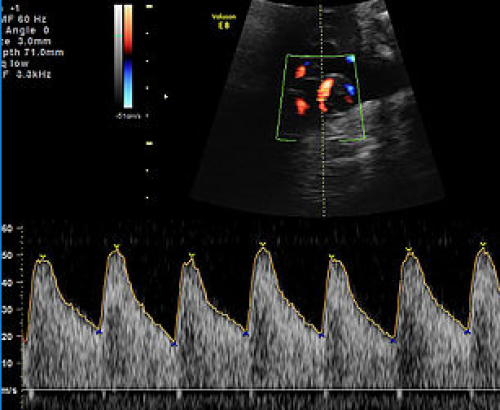
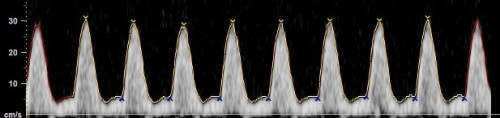
Normal MCA Doppler: High resistance with low diastolic flow velocities.
Abnormal: Low-resistance MCA waveform with high diastolic velocities.
Normal waveform with A wave above baseline.
Abnormal waveform: A wave below baseline and increased pulsatility.
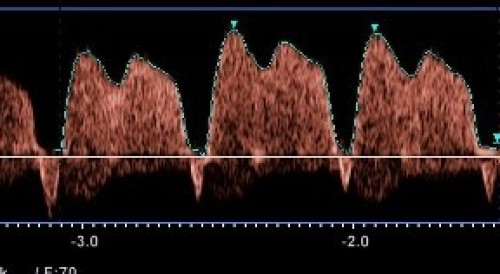
Normal low impedance / low resistance waveform with high diastolic flow and no notch.

Normal diastolic flow (normal impedance to flow) but early diastolic notching.
Abnormal waveform: Increased PI, with reduced diastolic flow and early diastolic notching.
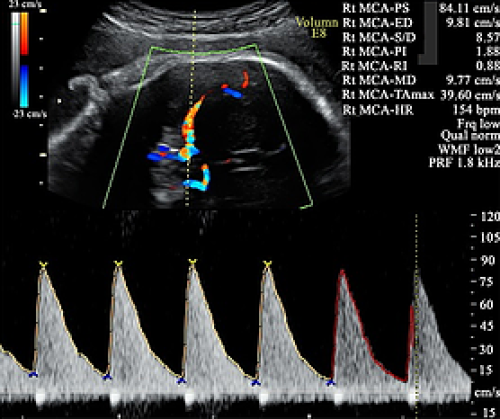
Elevated MCA PSV, well above 1.5 MoM.
Urgent
Same day