Twin Pregnancy
Twin Pregnancy scan guidelines
These guidelines were published in 2019 and are awaiting review, due 2022. Some content may be outdated.
Assessment of chorionicity and amnionicity (see below) is vital (first-trimester assessment is optimal).
Label the leading fetus ‘twin A’ and the following fetus ‘twin B’ and record position as left and right and upper and lower, by the relationship of each sac to the cervix, and assign gender if discordant.
Twins frequently change position: the description of fetal position must be clear, and state if the previously leading twin is no longer presenting; however, the labelling of twins A and B must not be changed during the pregnancy.
For further information, see Multiple Pregnancy (PDF, 318 KB) (NZMFMN 2015f).
Discordant CRL in monochorionic twins is associated with an increased risk of subsequent development of selective fetal growth restriction (sFGR).
Discordant NT in monochorionic twins may be associated with an increased risk of subsequent development of TTTS.
Because of the potential complications of monochorionic twinning, including TTTS, TAPS and sFGR, fortnightly scans are advised from 16 weeks gestation to delivery.
Every scan must include:
In the case of fetal demise of one fetus, there is a significant risk of ischemic brain damage in the surviving co-twin. A Fetal Medicine referral is needed.
Consideration should be given to magnetic resonance imaging (MRI) 6 weeks after the event, or longer depending on the gestation and parental wishes. Note: MRI is a tertiary-level decision.
| Stage 1 |
|
|---|---|
| Stage 2 |
|
| Stage 3 |
|
| Stage 4 |
|
There may be associated growth discrepancy and abnormal Doppler.
See Staging of twin-twin transfusion syndrome (Quintero et al 1999).
Raised MCA PSV (>1.5 MoM) indicating fetal anaemia in one twin and MCA PSV <1.0 MoM in the other.
Note: If only one MCA can be ascertained but it is between 1.0 and 1.5 MoM, then there is less concern to achieve the assessment of the second twin.
EFW discordance of >25 percent or EFW of one twin <10th centile.
Weight discordance is calculated as: (EFW larger twin – EFW smaller twin) / EFW larger twin.
Gratacos staging is used for sFGR (types I–III) (Bennasar et al 2017; Gratacos et al 2007).
Under the Guidelines for Consultation with Obstetric and Related Medical Services (Referral Guidelines) (Ministry of Health 2012), women with a multiple pregnancy should be under the care of a specialist obstetrician, though in many cases, care is shared with a midwifery LMC.
A specialist with an interest in high-risk pregnancy should be involved in the following situations:
Where there are ultrasound signs of TTTS, early referral within 24 hours to the regional Fetal Medicine unit is recommended for further assessment.
This condition can deteriorate quickly, and treatment for severe cases is available only in Auckland.
Emergency
Urgent
Same day
Chorionicity should be ascertained and clearly imaged for future reference at the earliest scan possible (ideally ≤14 weeks). If it is too early or not clear, a follow-up scan should be offered.
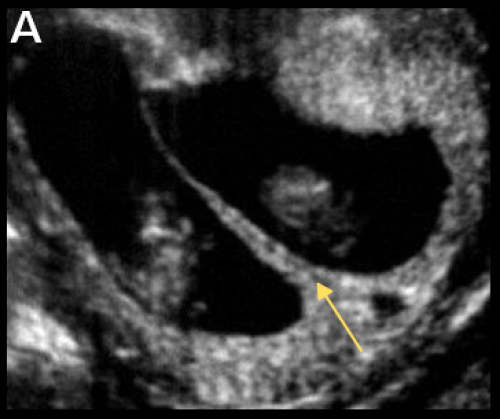
Lambda sign (arrow) indicating DCDA twin pregnancy.


T sign (arrow) indicating MCDA twin pregnancy (B) and absent intertwin membrane (C) in a MCMA twin pregnancy.
All twin pregnancies have increased rates of anomaly, preterm birth (both spontaneous and iatrogenic), pre-eclampsia, sFGR, GDM and complicated delivery, but the rate of complications is significantly increased in monochorionic (MC) twinning, due to placental anastomoses.