Cardiac anomalies
Cardiac anomalies guidelines
These guidelines were published in 2019 and are awaiting review, due 2022. Some content may be outdated.
The most common cardiac anomalies are summarised in this section.
The main reference source for this section is A Practical Guide to Fetal Echocardiography: Normal and abnormal hearts (Abuhamad and Chaoui 2015).
For more detail, please refer to this guide or another fetal echocardiography text.
VSDs are usually classified by their location. The most common VSDs identified prenatally are muscular and perimembranous.
VSDs may also be outlet or inlet in location. For more information, see Appendix 8: Anatomic locations of ventricular septal defects.
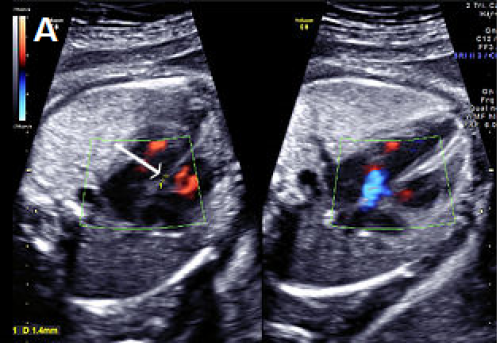
Small perimembranous VSD (arrow) on greyscale and colour Doppler imaging.
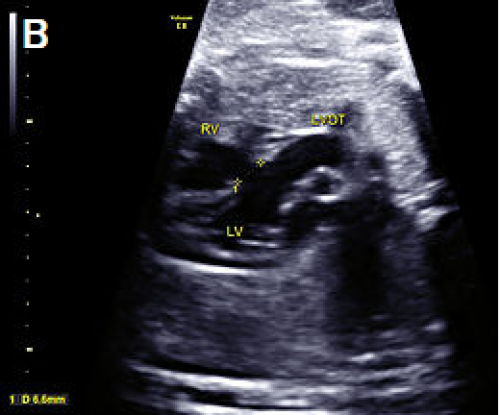
Larger VSD in the LVOT view, shown as discontinuity of the ventricular septum and aorta.

Perimembranous VSD on colour Doppler imaging.
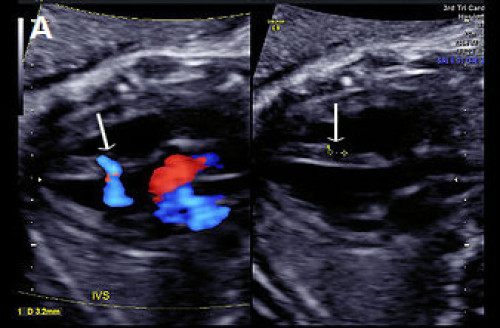
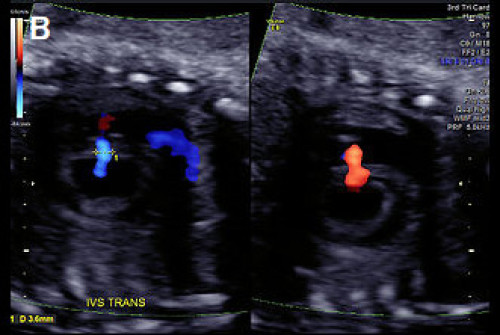
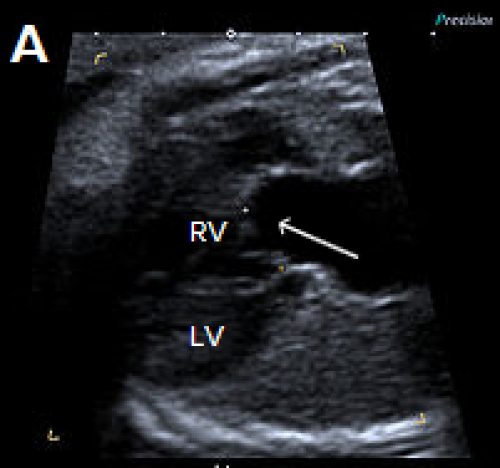
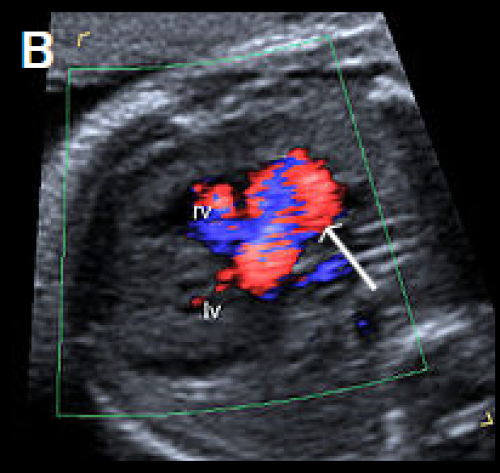
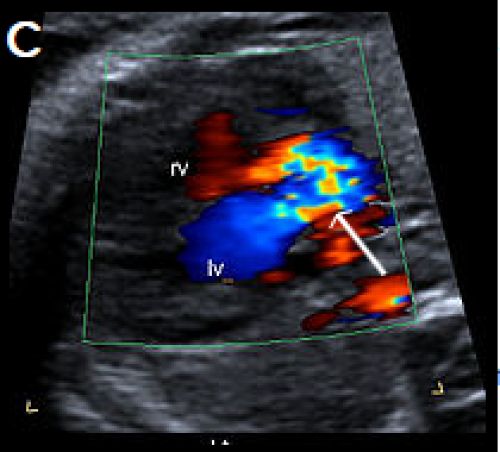
(A) Muscular VSD (arrow) on colour Doppler and greyscale imaging in the transverse long-axis IVS plane (arrows) and (B) in the transverse short-axis IVS plane with colour Doppler, showing bi‑directional flow.
AVSD may be complete or partial.
AVSD may be balanced or unbalanced (where the AV connection drains predominantly to one ventricle, causing disproportion in ventricular size).
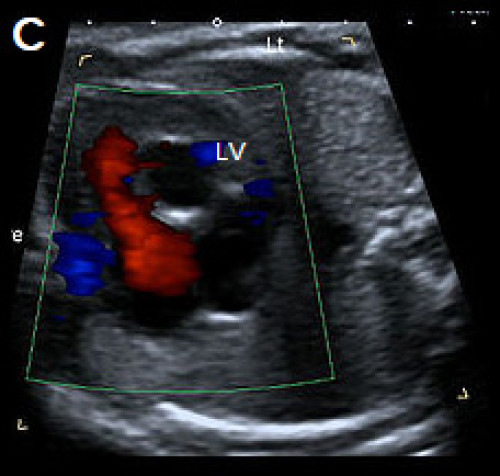
Colour Doppler is helpful in confirming the diagnosis, showing a single channel of blood flow to the ventricles, dividing over the remaining ventricular septum, and common valve regurgitation in most cases of complete AVSD.

Complete AVSD with common AV valve (arrow) in systole (valve closed).

Complete AVSD with common AV valve in diastole (valve open) with a large central defect (arrow).
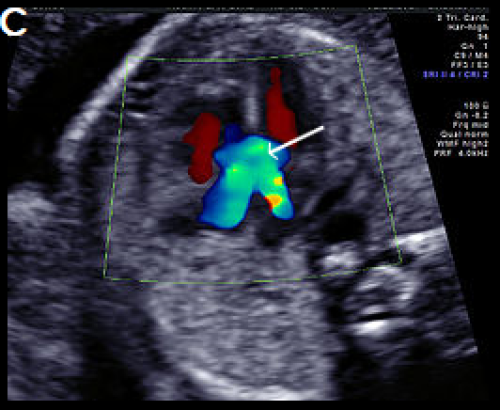
Complete AVSD with colour Doppler filling the large central defect and common valve regurgitation (arrow).
Classified according to embryonic origin and location as:
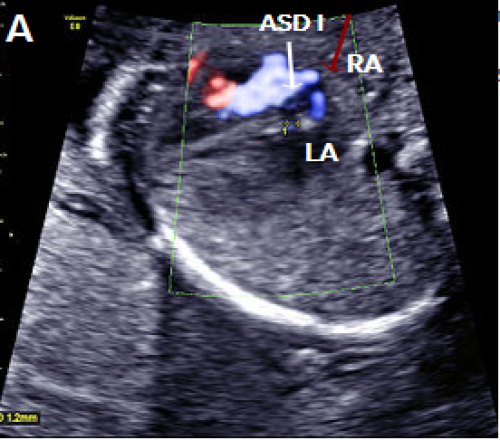
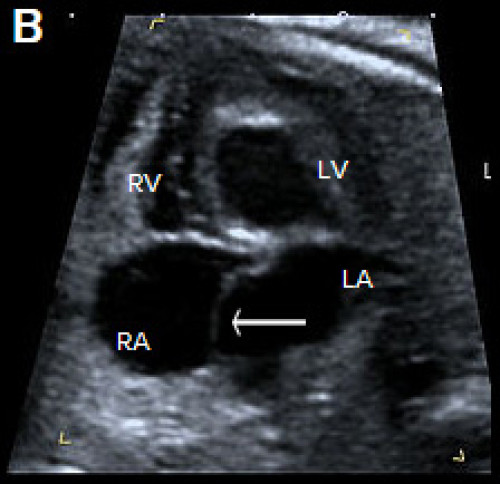
Septum primum ASD (white arrow) shown as a gap in the septum primum separate from the normal foramen ovale with right-to-left flow in blue (red arrow).
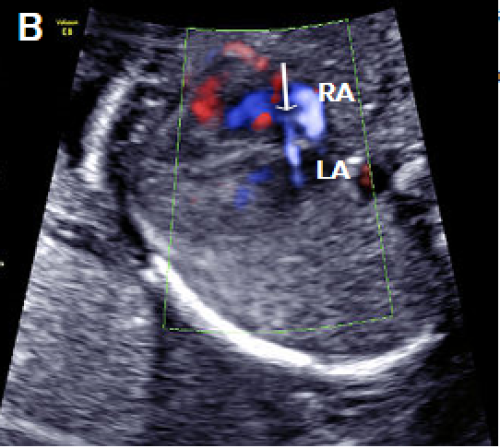
Septum primum ASD (white arrow), with right-to-left flow across the atrial septum (blue).
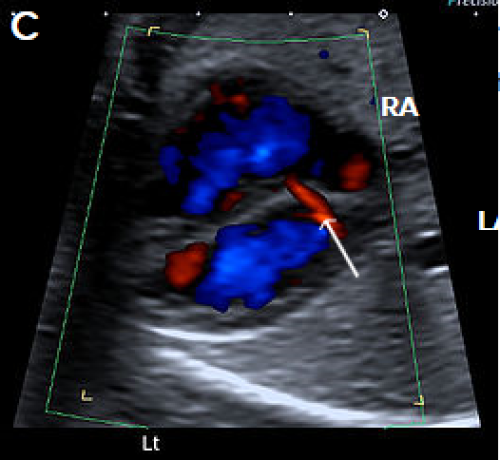
Normal coronary sinus (arrow) with left-to-right flow (red), which should not be misinterpreted as an ASD.
Tetralogy of Fallot (TOF) is one of the most common forms of cyanotic heart disease, occurring in about 1:3,500 live births.
TOF accounts for approximately 5 percent of cases of congenital heart disease.
TOF has three major prenatal components. These are:
The fourth component of the TOF is right ventricular hypertrophy and is usually not identified prenatally.
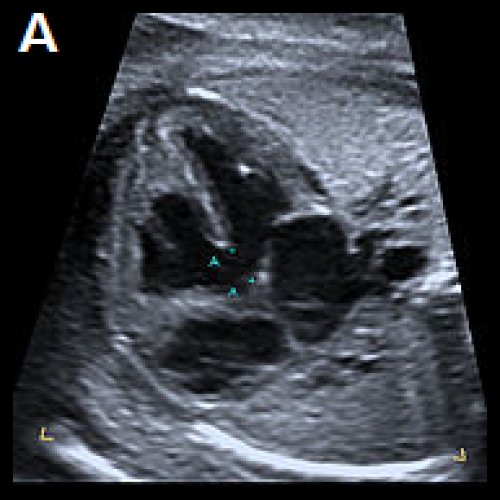
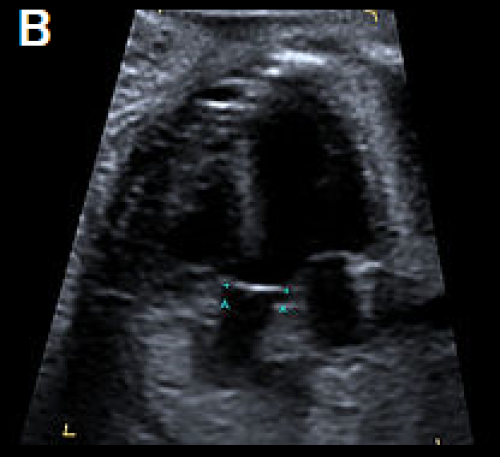
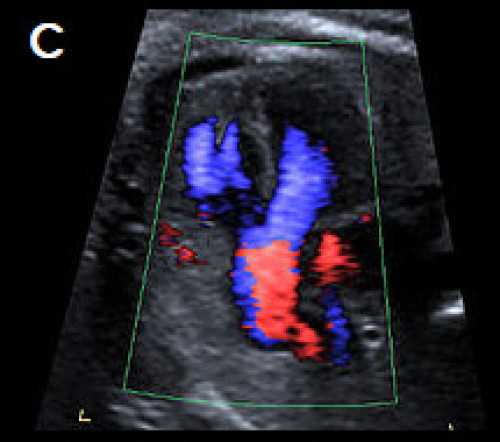
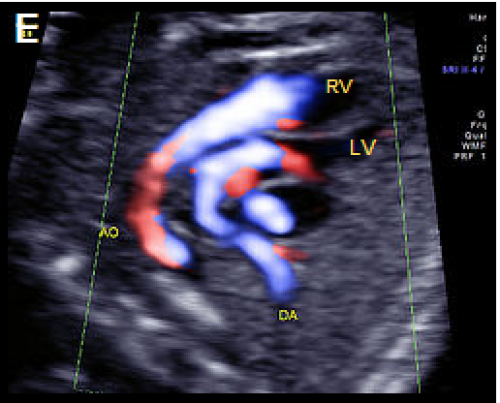
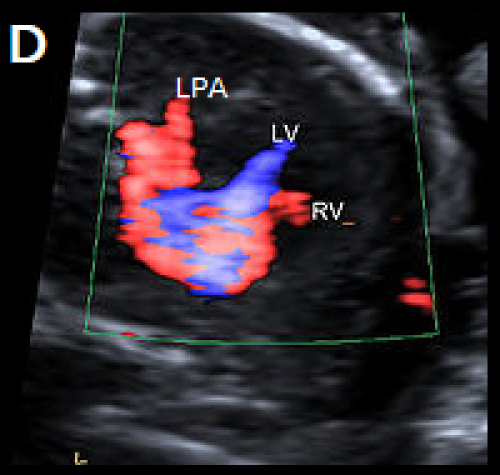
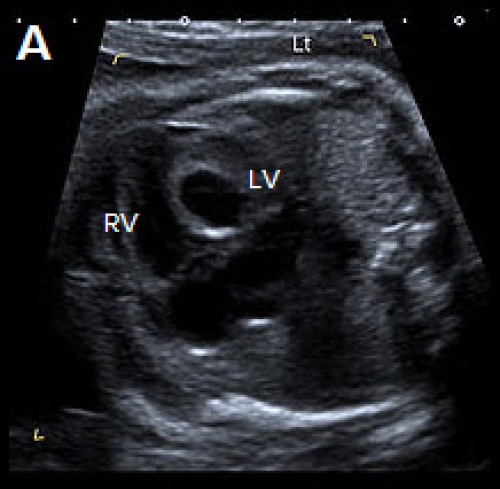
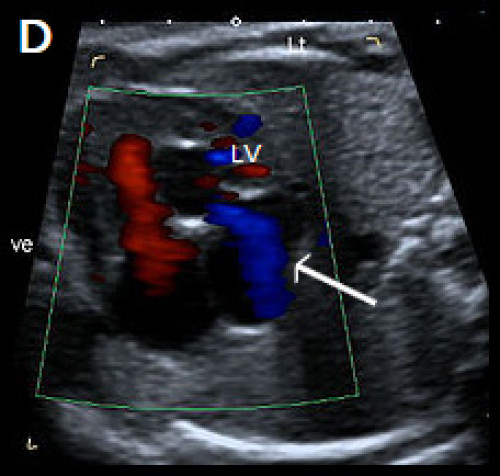
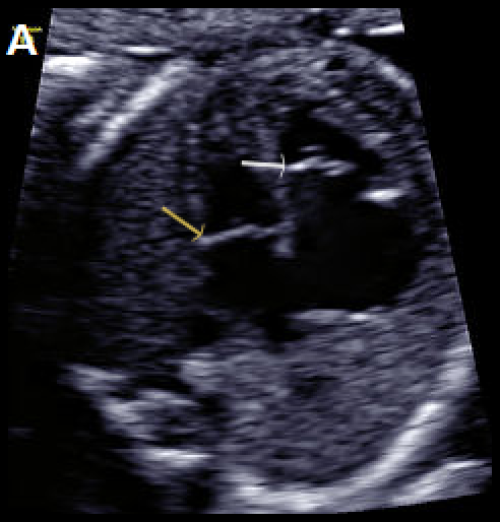
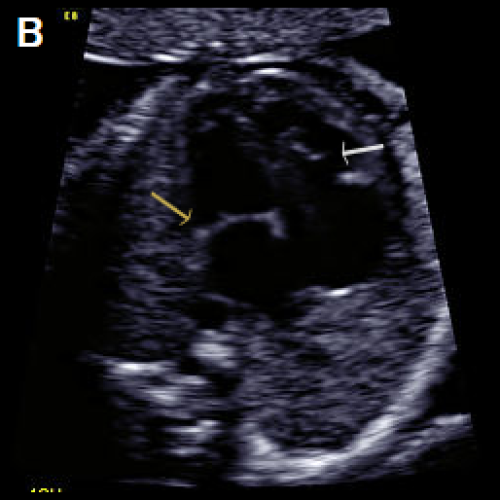
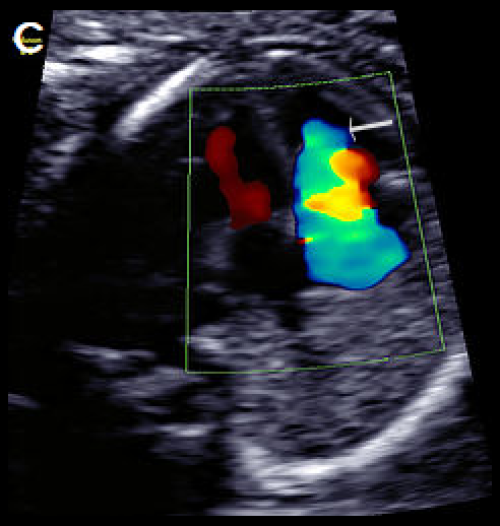
4Ch view (apex up) showing perimembranous VSD (A). Overriding, dilated aortic root with perimembranous VSD (B) and Y-sign with colour Doppler (blood from both ventricles flowing into the aortic root) on apex-up LVOT view in the same fetus (C).
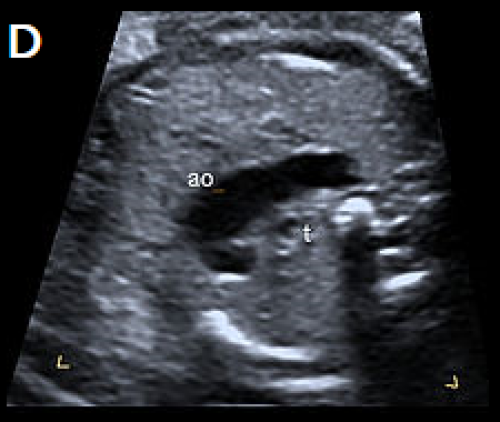
On the 3-vessel view only a single large vessel (the aorta) is evident in this case (D); colour Doppler may aid in demonstrating a small pulmonary artery.
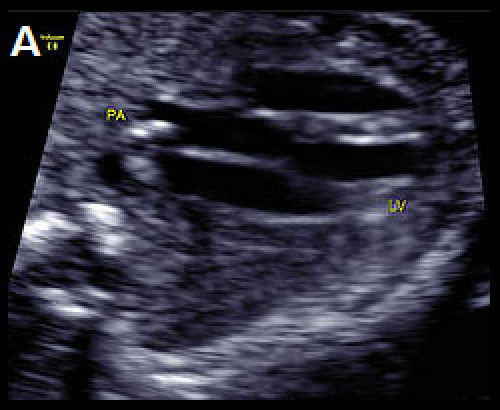
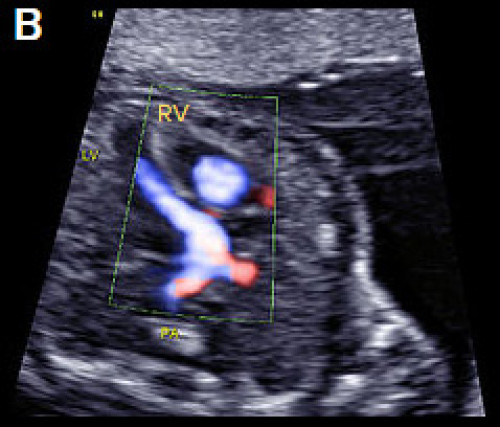
D-TGA with ventriculoarterial discordance. The bifurcating PA arises from the LV on the transverse long-axis LVOT plane, in B‑mode (A) and colour Doppler imaging, apex-up (B).
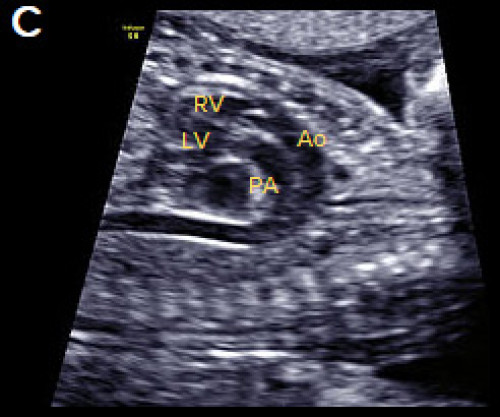
In the longitudinal plane, the aorta (Ao) with head and neck vessels arising from it, arises from the anterior RV, and the PA arises posteriorly from the posterior LV, on B-mode (C) and colour Doppler (D).
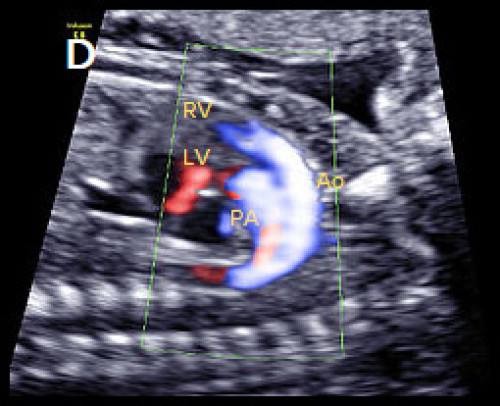
Oblique, apex-up view with colour Doppler showing the aorta arising from the (anterior) RV and the PA arising from the (posterior) LV.
Congenitally corrected TGA (cc-TGA) is a rare condition, with both AV and ventriculoarterial discordance (but normal veno-atrial connections).
Common arterial trunk (CAT) is also known as truncus arteriosus, persistent truncus arteriosus, truncus arteriosus communis and aorticopulmonary trunk. It is:
It may be classified into the following four types by the origin of the PAs, but this may be difficult prenatally.
A dysplastic truncal valve is common.
The following cardiac anomalies are commonly associated.
Extra-cardiac structural anomalies are present in about 40 percent of CAT cases.
Chromosomal anomalies are common, and include trisomies 21, 18 and 13 as well as microdeletion of 22q11.2 (in 30-40 percent of cases).

Single large central vessel (arrow) overriding both ventricles on greyscale (A) and colour Doppler imaging (B).
There is turbulent flow within the common arterial trunk on colour Doppler (C).
The left PA (D) and right PA, arrow (E), arise separately and distant from each other from the common arterial trunk (type 3 CAT).
Hypoplastic left heart syndrome (HLHS) comprises a spectrum of congenital anomalies characterised by under-development or absence of the LV and LVOT.
There are varying degrees of hypoplasia of the LV, mitral valve and aortic valve atresia or stenosis, and hypoplasia of the ascending aorta.
Critical aortic stenosis may progress to HLHS.
Abnormal small LV on the 4Ch view with an echogenic inner wall in keeping with endocardial fibroelastosis. The RV forms the apex of the heart (A).
Paradoxical left-to-right bulge of the foramen ovale flap, arrow (B). On colour Doppler imaging, there is minimal left ventricular filling (normal colour filling on the right, in red) (C), and mitral regurgitation, arrow (D).
Greyscale 4Ch view in a fetus with Ebstein anomaly showing mild cardiomegaly and apical offset of the septal tricuspid valve leaflet (white arrow), with ‘atrialisation’ of the RV.
Normal mitral valve position (yellow arrow), in diastole (A), with the same fetus in systole, with the valve leaflets open (B).
On colour Doppler imaging, there is a large tricuspid regurgitant jet arising from the mid-apical RV, (arrow) (C).
Beware: Severe fetal growth restriction may be associated with a narrowed isthmus due to shunting of blood and may be misinterpreted as coarctation.
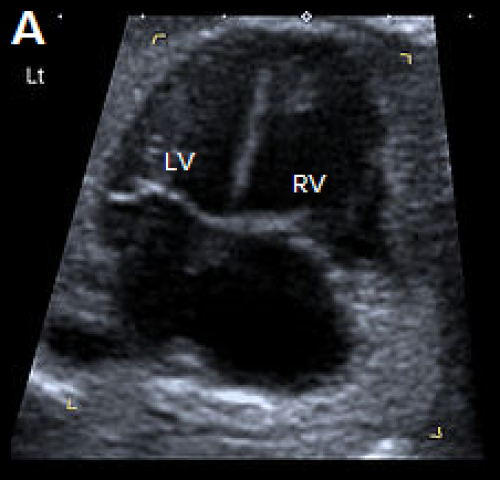
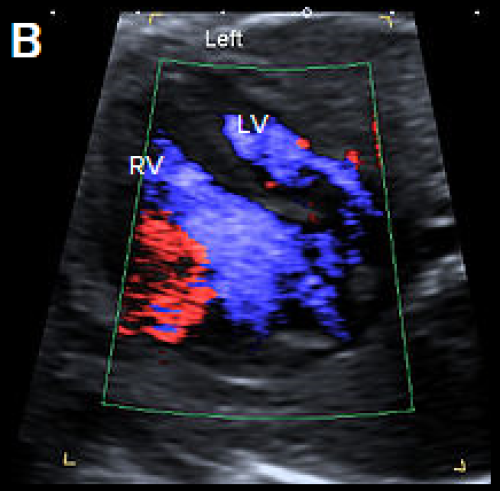
4Ch heart view showing narrower LV compared with the RV, on greyscale imaging (A), and with a narrower colour strip and patent AV valves on colour Doppler imaging (B).
3-vessel view in two different fetuses with coarctation (C) and tubular hypoplasia of the aortic arch (D), with a narrow aortic arch compared with the PA.
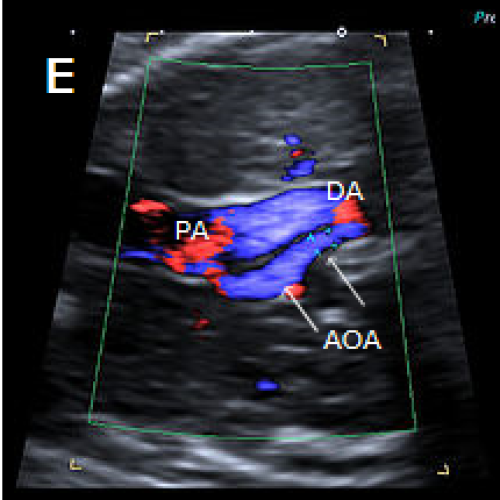
Colour Doppler confirms the narrow calibre of the aortic arch compared with the PA (E).
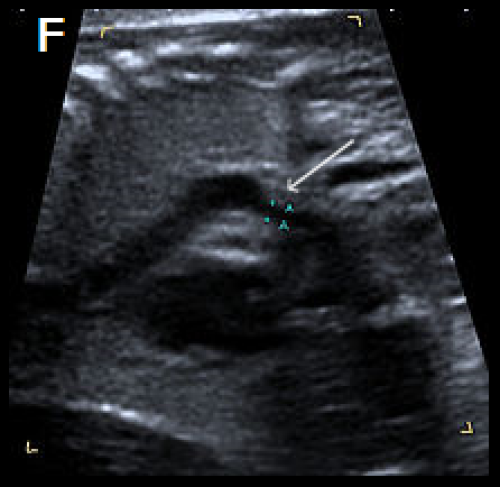
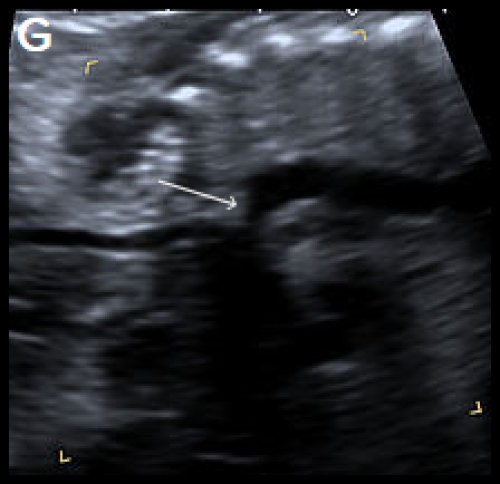
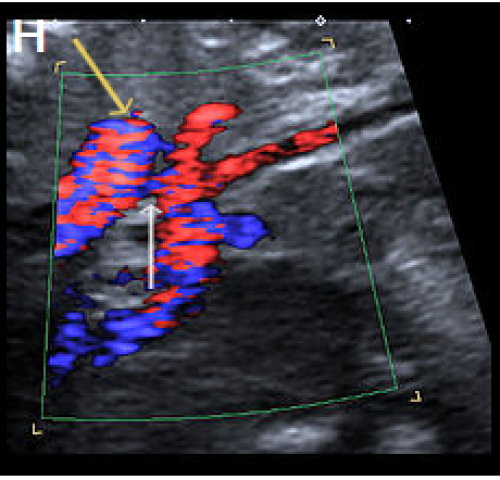
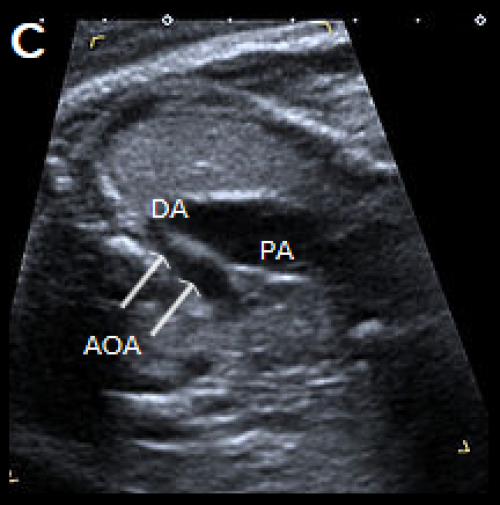
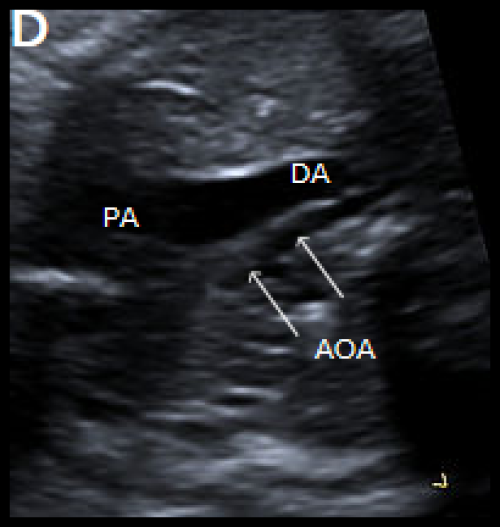
Sagittal views of the aortic arch in greyscale in two different fetuses, showing narrowing in the isthmic region (arrow) (F) and (G) and in colour Doppler (white arrow) (H), with the coarctation ‘shelf’ at the junction of the ductus and descending aorta (yellow arrow).
Interruption of the aortic arch (IAA) is a rare cardiac anomaly (comprising about 1 percent of CHD) in which there is incomplete development of the aorta, with a gap between the ascending and descending thoracic aorta.
It is almost always found in association with other cardiac anomalies, including VSD, aorto-pulmonary window and CAT at the junction of the ductus and descending aorta.
IAA may be classified by the anatomic location of the site of interruption as follows.
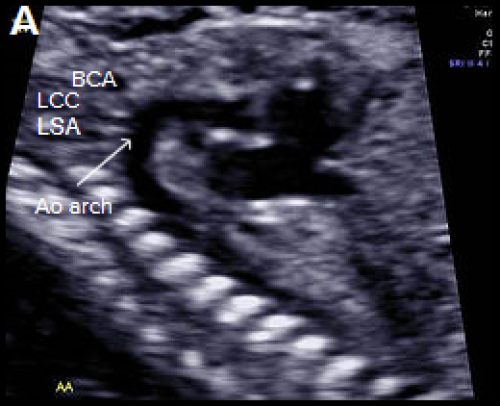
Longitudinal view of a normal aortic arch (A) showing the normal branching of the head and neck vessels. Brachiocephalic artery (BCA), left common carotid artery (LCC), left subclavian artery (LSA).
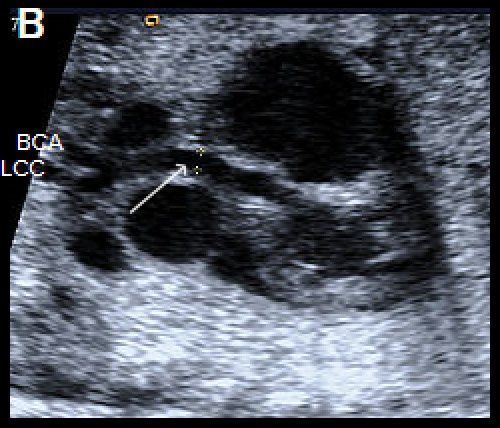
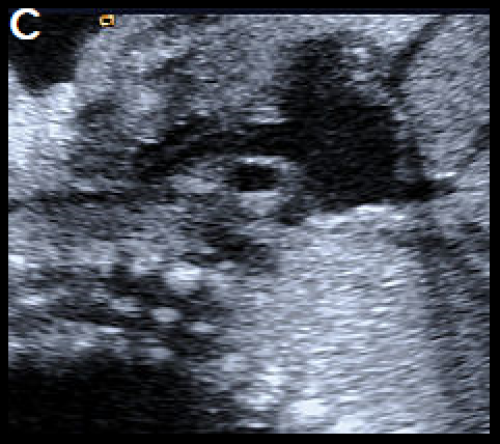
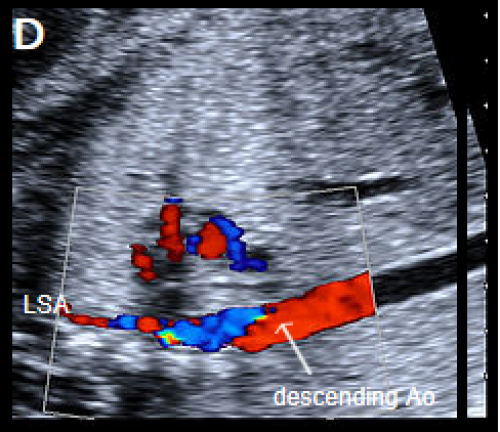
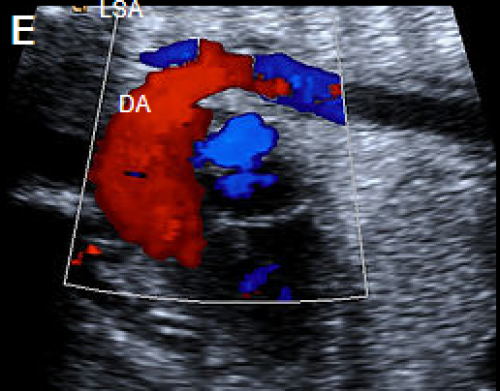
A fetus with IAA showing an elongated straight course of the small calibre aorta (arrow), continuing into the brachiocephalic and LCC arteries (B), and loss of continuity of the transverse arch in greyscale (C), and colour Doppler (D). The LSA arises from the ductus arteriosus (DA), (E).
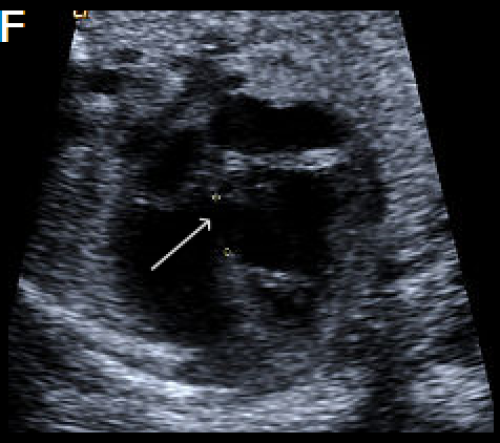
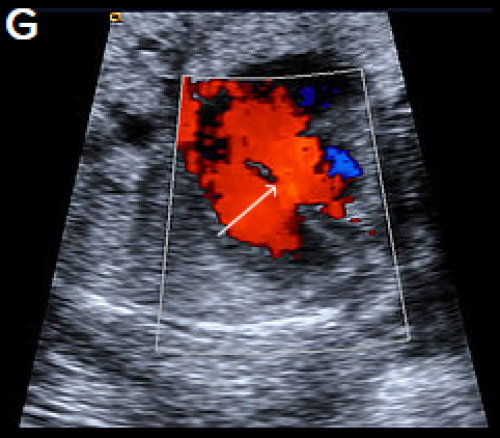
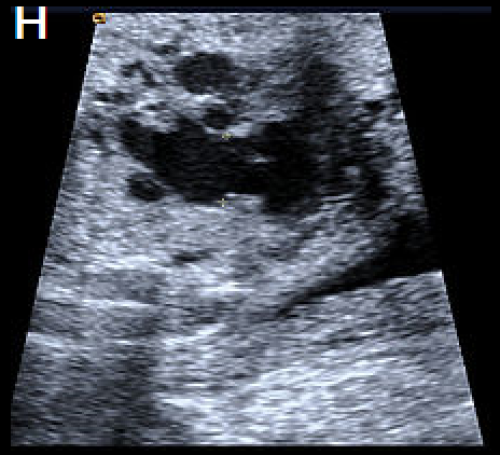
A perimembranous VSD is evident on greyscale (F), and colour Doppler (G), arrowed. Note that the ventricles are congruent in size. The RVOT appears dilated compared with the small aorta (H).