Pātiki and Waharua Kōpito patterns
On this page
- Key information
- 10.1. Virology and the causal link to cancer
- 10.2. Clinical features
- 10.3. Epidemiology
- 10.4. Vaccines
- 10.5. Recommended immunisation schedule
- 10.6. Contraindications and precautions
- 10.7. Potential responses and AEFIs
- 10.8. Cancer prevention measures
- 10.9. Variations from the vaccine data sheets
- References
Key information
|
Mode of transmission |
Skin-to-skin contact, predominantly sexual, with a person with human papillomavirus (HPV) infection. |
|---|---|
|
Period of communicability |
HPV infection is very common, with initial infection occurring soon after sexual debut and a lifetime risk of over 80%. Recurrent infection and co-infection with multiple types are possible. |
|
Incidence and burden of disease |
HPV is linked to almost all cervical cancers and to about 69% of vulvar, 75% of vaginal, 63% of penile, 90% of anal and 70% of oropharyngeal cancers. |
|
Funded vaccine |
HPV9 (Gardasil 9) is a recombinant subunit vaccine containing virus-like particles (VLPs). HPV9 contains HPV types 6, 11, 16, 18, 31, 33, 45, 52 and 58. |
|
Dose, presentation, route |
0.5 mL per dose. Pre-filled syringe. Intramuscular injection. |
|
Funded indications and recommended schedules |
2 doses, at 0 and 6–12 months for children aged 14 years and under. 3 doses, at 0, 2 and 6 months, for individuals:
An additional dose for individuals aged 9–26 years post-chemotherapy. NB: Individuals who were previously fully vaccinated with HPV4 are not eligible for HPV9. |
|
Vaccine effectiveness |
The incidence of HPV infection, precancerous lesions and genital warts is significantly reduced in immunised populations (in women and men). There is evidence for herd immunity (reductions in HPV infection and genital warts in unimmunised populations). |
|
Precautions and special considerations |
HPV vaccines are not recommended for pregnant women; however, enquiring about the possibility of pregnancy is not necessary before vaccination. |
|
Potential responses to vaccine |
Syncope (fainting) and other immunisation-related stress reactions are associated with giving vaccine to adolescents. |
|
Public health measures |
Measures for cancer prevention (see section 10.8):
|
10.1. Virology and the causal link to cancer
Human papillomaviruses (HPVs) are small, non-enveloped DNA viruses from the Papillomavirus family. There are about 150 different HPV serotypes. They vary in their preference for infecting squamous epithelium at different sites, thereby causing the various types of HPV infection (eg, common, palmar, plantar or anogenital). More than 40 HPV types can infect the anogenital tract.[1, 2]
Data from the US cancer registry indicates that HPV is causally associated with almost all cervical cancers, about 69 percent of vulvar, 75 percent of vaginal, 63 percent of penile, 90 percent of anal and 70 percent of oropharyngeal cancers (see Table 10.1).[3]
Based on their causal link to cancer, HPVs are divided into low-risk and high-risk types. There are approximately 12 high-risk types, which include 16, 18 and types 31, 33, 52, 58 and 45 that are genetically related to 16 and 18.[4] Types 16 and 18 are most frequently associated with cervical cancer but are also causally associated with other cancers. In the US, HPV types 16 and 18 are estimated to cause 66 percent of invasive cervical cancers, 80 percent of anal, 49 percent of vulvar, 55 percent of vaginal, 48 percent of penile and 60 percent of oropharyngeal cancers annually (Table 10.1).[3]
Low-risk types (especially types 6 and 11) are predominantly associated with non-malignant lesions, such as genital warts, and recurrent respiratory papillomatosis.
Table 10.1: Average annual percentage of cancer cases attributable to HPV, by anatomic site and sex, United States, 2008–2010
Table 10.1: Average annual percentage of cancer cases attributable to HPV, by anatomic site and sex, United States, 2008–2010
|
Anatomic sitec |
Cancers attributable to any HPVa, b |
Cancers attributable to HPV 16, 18a, b |
Cancers attributable to HPV 31, 33, 45, 52, 58a, b |
|---|---|---|---|
|
% |
% |
% |
|
|
Cervix |
90.6d |
66.2 |
14.7 |
|
Vulva |
68.8 |
48.6 |
14.2 |
|
Vagina |
75.0 |
55.1 |
18.3 |
|
Penis |
63.3 |
47.9 |
9.0 |
|
Anus |
|
|
|
|
92.5 |
79.5 |
10.8 |
|
88.7 |
79.1 |
3.8 |
|
Oropharyngeal |
|
|
|
|
63.3 |
50.8 |
9.5 |
|
72.4 |
63.4 |
4.4 |
|
a. Data is from 2008–2010 diagnosis years from population-based cancer registries that participate in the National Program of Cancer Registries and/or the Surveillance, Epidemiology, and End Results Program. b. These estimates do not consider future changes in incidence, population structure or the percentage of cancers that are HPV positive. c. International Classification of Diseases (ICD) codes: Cervix C53; Vulva C51; Vagina C52; Penis C60; Anus C21; Oropharyngeal (includes cancers of the soft palate, walls of pharynx, tonsils and base of tongue) C01.9, C02.4, C02.8, C05.1, C05.2, C05.9, C09.0, C09.1, C09.8, C09.9, C10.0, C10.2, C10.8, C10.9, C14.0, C14.2, and C14.8. d. Although HPV is accepted to be a necessary factor in the causal pathway to invasive cervical cancer, HPV is not always detected in tumour specimens from women who receive a diagnosis of invasive cervical cancer due to a variety of reasons, including misclassification of tissue specimens as cervix, quality of tissue specimens, assay sensitivity, and a small proportion of HPV-negative, cervical cancers.
Adapted from: Saraiya M, Unger ER, Thompson TD, et al. 2015. US Assessment of HPV types in cancers: Implications for current and 9-valent HPV vaccines. Journal of the National Cancer Institute 107(6), DOI: 10.1093/jnci/djv086 Table 4. |
|||
10.2. Clinical features
10.2.1. Infection
10.2.1. Infection
Infection results from predominantly sexual skin-to-skin contact with a person with HPV infection. Transmission in the genital region may occur even when condoms are used and does not necessarily require penetrative intercourse. HPV may also be transmitted perinatally from mother to newborn baby.
Clinically apparent warts are probably more infectious than subclinical infection. The virus penetrates micro-abrasions in the epithelium to reach the basal epithelial cells, where it causes the infected cells to produce proteins that delay cellular maturation. Continued replication of these infected cells in the intermediate epithelial layer, followed by virus replication in the superficial epithelial layer, results in the cellular overgrowth typical of warts.
For most people, HPV infection is transient and becomes undetectable by DNA testing within 6 to 12 months, but in some cases, HPV infection remains latent and may reactivate years later. As it is difficult to detect HPV in its latent stage, it is impossible to know whether the immune system can completely clear the virus or whether, in some cases, undetectable latent virus is capable of later re‑emerging.
Acquisition of HPV
Infection with oncogenic serotypes of HPV is common, with an estimated 70–80 percent of sexually active individuals becoming infected at some stage during their life. Initial infection occurs soon after sexual debut.
Most episodes of infection become undetectable by DNA testing within two years of acquisition; the average duration of infection is one year. Previous infection does not necessarily create long-term immune memory so does not prevent future re-infection with the same HPV type.
At any one time, approximately 10 percent of women have at least one HPV infection. The HPV serotypes that cause more prolonged infection tend to be those that more frequently result in the development of histological abnormalities.[5, 6]
Two US studies found that incidence of genital HPV infection was higher in men than for similar cohorts of young women. In university students (age 18–20 years), the cumulative incidence of first-time infection at 24 months was 32 percent (95% CI: 28.0–37.1) for females compared with 62.4 percent (95% CI: 52.6–72.2) in heterosexually active male students. Frequent new sexual partners and a history of smoking were associated with an elevated risk of HPV acquisition for both.[7, 8]
There are differences between the sexes in the immune response to HPV. A smaller proportion of men are HPV-seropositive, and men have lower antibody titres than women.[9] In contrast to women, for whom the risk for HPV acquisition increases with age through the early 20s and then decreases, studies have demonstrated HPV prevalence in men seems to peak at slightly older ages and remains constant or decreases slightly with increasing age, suggesting persistent HPV infection or a higher rate of re-infection.[10, 11]
Men who have sex with men, especially those who are HIV-positive, are at higher risk for HPV infection, anal cancer and high-grade anal intraepithelial neoplasia.[12] In teenage men who have sex with men (aged 16–20 years), early and high per-partner HPV transmission occurs between men soon after their first sexual experiences.[13]
Individuals who are immunocompromised (due to medical conditions or treatment) are more likely to develop a persistent HPV infection and to subsequently progress to HPV-related disease.[14, 15] Those with confirmed HIV infection are more at risk of HPV infection.[16] HPV is less likely to become undetectable in individuals coinfected with HIV.[17, 18] A direct relationship has been identified between low CD4+ cell count and an increased risk of cervical cancer in HIV-infected women.[19]
10.2.2. Cervical cancer
10.2.2. Cervical cancer
HPV rapidly becomes undetectable in the first 6–12 months of acquisition of infection, with 80–90 percent undetectable by two years. Following this, a very small fraction of persistent infection progresses to cervical intraepithelial neoplasia (CIN); these are non-invasive precancerous lesions, which are categorised as either low- or high-grade CIN. Invasive cervical cancer occurs when the lesions invade the cervical tissue, and is graded from stage I to IV, depending on how far the cancer has spread beyond the cervix into surrounding tissue or organs.
Cervical cancer does not usually develop until decades after acquisition of infection with an oncogenic (cancer-causing) HPV serotype. Persistent HPV infection is detected in almost all women with cervical cancer.[20]
HPV infection is essential, but not sufficient by itself, for the development of cervical cancer. Other factors have been described that may be associated with HPV persistence and high-grade lesions including smoking, early onset sexual activity, older age, contraceptive use, multiple sexual partners and genetic factors.[21, 22]
10.2.3. Oropharyngeal and other cancers
10.2.3. Oropharyngeal and other cancers
The clinical features of other HPV-associated cancers and their precancerous lesions in the anogenital and oropharyngeal regions vary, and also depend on the anatomical site. The progression from HPV‑associated precancer lesions to cancers in these sites is less well understood than the process in the cervix.
Oropharyngeal cancers include cancers of the soft palate, the walls of the pharynx, the tonsils and the base of the tongue. The risk factors for oropharyngeal cancer are similar to those for cervical cancer, including the number of sexual partners, younger age at first sexual intercourse, practice of oral sex, history of genital warts and younger age.[23]
10.2.4. Genital warts and recurrent respiratory papillomatosis
10.2.4. Genital warts and recurrent respiratory papillomatosis
HPV 6 and 11 account for around 90 percent of all genital wart cases. Most warts cases are self-limited, although some may persist for several years. Persistence is more common in patients with impaired cell-mediated immunity.[2]
Perinatal transmission of HPV (usually types 6 or 11) can cause laryngeal infection in infants, which in rare cases can result in recurrent respiratory papillomatosis in children. Respiratory papillomatosis is characterised by multiple warty growths on the mucosal surface of the respiratory tract, which can cause hoarseness and significantly obstruct the airways and require repeated surgery.[2]
10.3. Epidemiology
10.3.1. Global burden of disease
10.3.1. Global burden of disease
HPV is an important carcinogenic infection. The 12 high-risk types are reported to be the second most common infectious cause of cancer worldwide after Helicobacter pylori.[24] It has been estimated that 4.5 percent of all cancers (630,000 new cancer cases per year) are attributable to HPV; over 70 percent are attributable to HPV types 16 and 18, and 90 percent to types contained within the HPV9 vaccine. The greatest burden is in India and sub-Saharan Africa, where there is limited access to both screening and vaccination, and more than 20 percent of cancers in women are attributable to HPV infection.[25]
Onset of sexual activity
Most HPV infections occur within the first two years of onset of sexual activity; more than 40 percent of individuals become infected during this period. The first sexual relationship carries a substantial risk.[26]
Cervical cancer
Cervical cancer is the fourth cause of female cancer and cancer deaths in the world and is the second most common cause of female cancer and cancer deaths in women aged 15–44 years; the estimated incidence rate of cervical cancer cases attributable to HPV across Oceania was 10.1 (range 5.6–28.3) per 100,000 across all ages; the estimated annual mortality was 4.6 (range 1.6–18.6) per 100,000 in 2020.[27]
Persistent HPV infection can lead to high-grade CIN. Approximately one-third of CIN3 progresses to invasive cervical cancer within 10–20 years. A 2010 study reported that more than one-quarter (26.7 percent; 95% CI: 21.1–31.8) of those with persistent HPV16 and nearly one in five (19.1 percent; 95% CI: 10.4–27.3) of those with persistent HPV18 developed CIN3 or cancer within 12 years.[28] A multi-national study across 38 countries found HPV types 16, 18, 31, 33, 45, 52 and 58 in 85 percent of invasive cervical cancer cases, 71 percent (95% CI: 70-72) of cervical adenocarcinomas were positive for HPV16 and 18 and 94 percent (95% CI: 92-96) were positive for HPV16, 18 and 45.[20]
Other HPV-related cancers
Oncogenic HPV types are linked to other cancers in women and men, including vulval, vaginal, penile, anal and oropharyngeal cancers (see Table 10.1).
Anal cancers
Anal cancer remains relatively rare compared to other cancers, but the global incidence has increased among both men and women, particularly in high-income regions (the average worldwide incidence is 0.5 per 100,000 population in 2020).[27] Women have a higher incidence of anal cancer than men. The incidence is highest among men who have sex with men, women with history of cervical or vulvar cancer, and immunosuppressed populations, including those who are HIV-infected and patients with a history of organ transplantation.[27]
Oropharyngeal cancers
There has been an increase in the incidence of head and neck cancers over the past few decades. This increase is mainly due to an unexpected increase in HPV-related oropharyngeal cancers, primarily in males aged 40–55 years with exposure to alcohol and tobacco.[29]
Most recent data suggest that around one-quarter of all oropharyngeal cancers are attributable to HPV infection; the most frequent type is HPV16.[25, 27] (see Table 10.1).
Vulval and vaginal cancer
Vulval and vaginal cancers are rare worldwide, representing 4 percent and 2 percent of all gynaecological cancers. Incidence is highest in less developed countries.[27]
Genital warts
Genital warts, which are most commonly due to infection with HPV6 or HPV11, have a prevalence of approximately 1 percent of adults in the US.[30,31] Scandinavian countries have reported rates as high as 10 percent.[32]
10.3.2. New Zealand epidemiology
10.3.2. New Zealand epidemiology
Onset of sexual activity
Data from the Youth’12 survey suggests that approximately 8 percent of New Zealand adolescents may have had sexual intercourse before the age of 13 years.[33, 34] This increases to 24 percent by the age of 15 years and 46 percent by age 17 years.
Compared to 2001, students were more likely to delay sexual debut in 2012 but less likely to use condoms and contraception consistently.[35] Māori (OR 0.7; 95% CIs: 0.6–0.8) and Pacific (OR 0.5; 95% CIs: 0.4–0.7) students used condoms less frequently than NZ European students; those from socioeconomically deprived communities (school decile 1) used condoms less frequently (OR 0.7; 95% CIs: 0.5–0.9) than students from wealthier communities (school decile 10).[35]
Cervical cancer
HPV prevalence in precancerous lesions and invasive cervical cancer
The prevalence of HPV infection and distribution of HPV types among New Zealand women with histologically confirmed CIN 2/3[36, 37] or invasive cervical cancer[38] was broadly consistent with that seen internationally. During 2011–2012, 97 percent (95% CI: 94–98) of women with histologically confirmed CIN 2/3 were HPV-positive, and the prevalence of any high-risk HPV was 96 percent (95% CI: 91–99).[36] In women with histologically confirmed invasive cervical cancer during 2004–2010, 88.5 percent (95% CI: 83.7–92.4) were HPV-positive, and the prevalence of any high-risk HPV was 87.2 percent (95% CI: 82.2–91.3).[38] For both CIN 2/3 and invasive cervical cancer, the overall distribution of HPV types was similar in Māori and non-Māori women, with HPV16 being the most commonly detected HPV type in both groups.[36, 38]
Cervical cancer registrations and deaths
In 2018 (provisional), there were 191 new cervical cancer registrations, an increase from 164 in 2017.[39] In 2017, the age-standardised registration rate was 6.0 per 100,000 population, similar to the 2016 rate (6.4 per 100,000). The registration rate for Māori women was 9.4 per 100,000, 1.7 times greater than the rate for non-Māori women (5.4 per 100,000).[39]
There were 55 cervical cancer deaths in 2016. In 2014, when there were 46 deaths (1.4 deaths per 100,000 population) and the mortality rate for Māori women was 3.0 per 100,000, 2.7 times greater than for non-Māori women (1.1 per 100,000).[40]
Other HPV-related cancers
The most recent New Zealand data available for other HPV-related cancers is from 2017 (see Table 10.2). Note that this data is for new cancer registrations only; the tumours have not been analysed for the presence of HPV.
Table 10.2: Number and age-standardised rate of new registrations for other cancers known to be associated with HPV in New Zealand, 2017
|
Anatomic site* |
Number of new registrations |
Rate of new registrations |
|---|---|---|
|
Vulva |
52 |
1.2 |
|
Vagina |
19 |
0.5 |
|
Penis |
18 |
0.5 |
|
Anus |
|
|
|
40 |
1.1 |
|
21 |
0.6 |
|
Oropharynx |
|
|
|
4 |
0.1 |
|
10 |
0.3 |
|
Tonsils |
|
|
|
21 |
0.6 |
|
85 |
2.7 |
|
* ICD codes: Vulva C51; Vagina C52; Penis C60; Anus C21; Oropharynx C10; Tonsils C09. (Note that in Table 10.1, the US definition for oropharyngeal cancer combines multiple cancers, using 4-character ICD codes. At the time of writing, New Zealand data for 2017 was only available at the 3-character ICD code level.)
Source: Ministry of Health. 2019. New cancer registrations 2017 (external link). Wellington: Ministry of Health (accessed 20 June 2020). |
||
Anal cancers
For the period 2008–2012, the age-standardised rate for anal cancer was 0.6 and 1.1 per 100,000 persons per year among men and women in New Zealand, respectively.[27] It remained the same in 2017 (see Table 10.2).
Oropharyngeal cancers
A retrospective review of New Zealand cancer registry data for the period 1981–2010 showed a rapid rise in oropharyngeal cancers in men (mainly in those aged 40 years or older), particularly from 2005 onwards.[41] The rate of oropharyngeal cancers was almost four times greater in men (1.87 per 100,000) than in women (0.47 per 100,000). The incidence rates for oral cavity cancer, which is generally associated with alcohol and tobacco consumption, remained relatively stable in both sexes during that time. (Note that this study included both oropharyngeal and oral cavity cancers.)
A significant increase in HPV-positive oropharyngeal cancer (OR 5.65; 95% CI: 2.60–12.30 was detected in biopsies taken during 1996-1998 and 2010-2012 and occurring at a younger age (OR 0.55; 95% CI: 0.33-0.99 aged 61 or older and age 60 years or younger). Most cases attributable to HPV were HPV16-positive (98.5 percent); there was also one case each of HPV 33 and 35.[42]
Genital warts
Many sexually transmitted infections (STIs), including genital warts, are not notifiable in New Zealand. ESR cautions that the number of cases of genital warts reported through the clinic-based surveillance system likely underestimates the true burden of disease in New Zealand because a substantial percentage of STIs are diagnosed by other health care providers.
Following the introduction of HPV4 vaccine to females in 2008 and the introduction of HPV9 vaccine for males and females in 2017, from 2008 to 2019 genital warts clinical case counts reported by sexual health clinics have decreased by 79.5 percent (from 3,681 to 756 cases) and case counts reported by family planning clinics decreased by 77.8 percent (from 573 to 127 cases) (ESR 26 June 2020). Since the introduction of the HPV vaccination programme, there have been decreases in the number of genital warts diagnoses in all ethnic groups in sexual health clinics and in all ethnic groups, except ‘Other’, in family planning clinics.
In sexual health clinics, the decrease was most notable in the 15–19 years and 20–24 years age groups, and there was a moderate decrease in the 25–29 years age group, in both sexes (Figure 10.1). A marked decrease was following the extension of vaccination to males in 2017. From 2016 to 2019, reported cases decreased by 50 percent (from 28 to 14 cases) in the younger males aged 15–19 years and 45.3 percent (from 190 to 104 cases) in those aged 20–24 years (ESR, 26 June 2020). A decrease in cases seen in older age groups suggests that immunisation is also providing some herd immunity to unvaccinated individuals. A decline in the number of prescriptions for treating genital warts (imiquimod and podophyllum resin-based products) supports this evidence for a herd immunity effect.[43] The largest decline was seen in women aged under 20 years.
A study in Auckland sexual health clinics found a similar population effect in genital wart cases over five years following the introduction of HPV4 to women in 2009. A significant reduction in new genital warts cases was observed in a vaccine-eligible age group of females (aged< 20 years), not observed in older age-groups (those aged over 20 years) or in males, not eligible to vaccination at that time. There was a smaller but not statistically significant decrease in genital warts cases in younger males (age <20 years) compared with that seen in older males.[44]
Figure 10.1: Number of genital warts (first presentation) in sexual health clinics, by sex and age group, 2008–2019
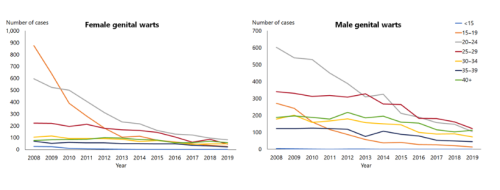
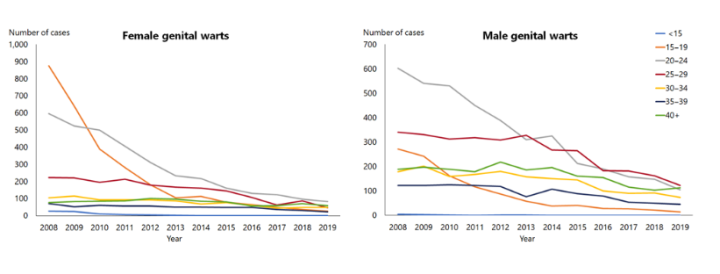
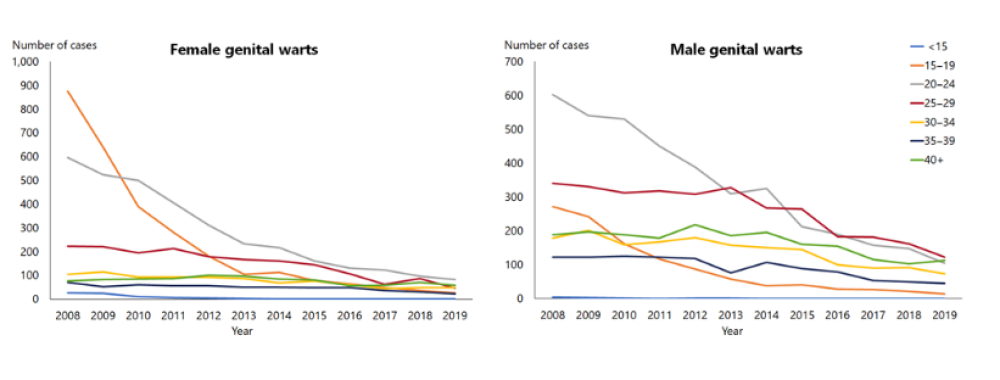
Source: ESR
For further details of genital wart notifications, refer to the most recent STI quarterly and annual reports from ESR (external link).
10.4. Vaccines
10.4.1. Available vaccines
10.4.1. Available vaccines
One HPV vaccine, HPV9 (Gardasil 9, Seqirus/MSD), is approved for use (registered) and is available for distribution (marketed) in New Zealand.
HPV9 is registered for use in females and males aged 9–45 years as a two-dose schedule in individuals aged 14 years and under, and as a three-dose schedule in older individuals and immunocompromised individuals from age 9 years.
The vaccine contains HPV virus-like particles (VLPs), which are composed of the L1 protein (a component of the virus outer layer) aggregated into clumps that mimic the outer structure of the HPV virion. The VLPs do not contain viral DNA and are incapable of causing infection. The L1 proteins are produced by genetically engineered yeast cells.
Funded HPV vaccine
Each 0.5 mL dose of HPV9 vaccine (Gardasil 9, Seqirus/MSD) contains:
- 30 µg of HPV6 L1 VLP, 40 µg of HPV11 L1 VLP, 60 µg of HPV16 L1 VLP, 40 µg of HPV18 L1 VLP, 20 µg of HPV31 L1 VLP, 20 µg of HPV33 L1 VLP, 20 µg of HP45 L1 VLP, 20 µg of HPV52 L1 VLP and 20 µg of HPV58 L1 VLP
- 500 µg of aluminium hydroxyphosphate sulphate.
The vaccine does not contain any preservative or antibiotics.
Other vaccine
HPV4 (Gardasil) was used prior to the introduction of HPV9 (Gardasil 9) in January 2017. See also section A1.3.4 in Appendix 1 for the history of HPV vaccines in New Zealand.
In other countries, including Australia and in Europe, a bi-valent HPV vaccine (Cervarix, GSK) is available to protect against HPV types 16 and 18 only. This vaccine is unavailable in New Zealand.
10.4.2. Efficacy and effectiveness
10.4.2. Efficacy and effectiveness
Most HPV vaccine clinical trials do not collect direct data about clinical outcomes, like cancer or precancer, for young adolescents, because it is unethical to collect samples from the cervix of vaccinated girls who are sexually naïve and because precancerous lesions do not appear for years after the HPV infection has occurred. Also, since treatment is offered as precancers develop, progression to cervical cancer is rare even in those not vaccinated and requires a very long time for follow-up. Therefore, immunological bridging is used to infer efficacy against cervical and anal cancer. Efficacy is also inferred for the younger age group because immunogenicity (antibody responses) is non-inferior to that seen in older age groups.
Immunogenicity
Although there is no known correlate of protection (ie, an established antibody level required for protection against HPV-related disease), HPV vaccines generate excellent antibody responses in most recipients.
HPV4
Immunisation with three doses of HPV4 vaccine produces antibody responses against HPV16, HPV18, HPV6 and HPV11 in more than 99 percent of vaccine recipients. The peak antibody titres following three doses of HPV vaccine are greater than that following natural infection.
A Cochrane systematic review found the immunogenicity of two- and three-dose HPV vaccination schedules in young females to be comparable.[45] Two doses of HPV4 are more immunogenic in recipients aged between 9 and under 15 years than in older groups aged over 15 years and comparable to three doses in older recipients (those over 15 years).[46] In young females, two doses have been found to be non-inferior to three doses for at least 21 months after vaccination, particularly when the interval between doses is at least six months.[47, 48] The immunogenicity of three doses of HPV4 vaccine has been established to be robust and long-lasting.[49,50,51] Anamnestic responses have been demonstrated out to at least 8.5 years.[51]
Differences in seroconversion rates and antibody titres were seen in immunocompromised individuals. The immune response to HPV4 among immunocompromised children appears adequate,[52,53] although antibody titres were lower than those in healthy children of the same age groups.[52] Seroconversion among HIV-infected individuals has been demonstrated to be robust and higher among those with lower HIV loads or on antiretroviral therapy.[54,55,56]
While some immunosuppression regimes can attenuate the immune response to HPV4, patients with autoimmune diseases generally appear to respond well to the vaccine.[57] In contrast, adult solid organ transplant recipients produce suboptimal responses to HPV4.[58]
HPV9
The immunogenicity of HPV9 vaccine was initially assessed in women aged 16–26 years.[59] Antibody responses generated by the HPV9 were non-inferior to HPV4 against HPV types 6, 11, 16 and 18; and in girls and boys aged 9–15 years.[60] Antibody responses to all nine vaccine HPV types in girls and boys aged 9–15 years and men aged 16–26 years were non-inferior to women aged 16–26 years.[61,62]
Men who have sex with men appear to produce lower antibody titres than heterosexual men (although seroconversion rates to all nine vaccine types were greater than 99 percent in both groups).[61] This lower antibody response is possibly due to greater exposure to the virus, highlighting the importance of vaccination at a young age.
The immunogenicity of two doses of HPV9 in girls and boys aged 9–14 years was non-inferior to three doses in women aged 16–26 years, the age group in which efficacy was demonstrated.[63]
Efficacy
HPV-related cancers
HPV4 and HPV9 vaccines offer similar protection against cervical, vaginal and vulval precancerous lesions or cancer in women vaccinated at 15–26 years.[45] Protection is greatest among young women not initially infected with HPV 16/18 prior to vaccination (vaccine efficacy of 95 percent [95% CI: 83–99] against vaginal and vulval lesions).[64]
HPV9 efficacy was studied in women aged 16–26 years and compared with HPV4.[59] HPV9 prevented cervical, vulvar and vaginal disease and persistent infection related to HPV types 31, 33, 45, 52 and 58 (the five additional serotypes in HPV9). The antibody response and incidence of disease related to HPV types 6, 11, 16 and 18 were similar in the two vaccine groups.
Protection against CIN 2/3 or adenocarcinoma in situ is widely accepted as a surrogate for protection against invasive cancer, since study participants who develop these precancerous lesions require treatment to prevent progression to invasive cancer. Bivalent and quadrivalent HPV vaccines have been shown to be highly effective in preventing these HPV16- and HPV18-related precancerous lesions in females.[1,65] In the pivotal efficacy trial in women aged 15–26 years, HPV4 vaccine efficacy for the prevention of precancerous lesions related to HPV16 or HPV18 was 98 percent (95% CI: 86–100) in the per-protocol susceptible population.[66]
A phase III clinical trial among Asian and Latin American women found population-specific vaccine efficacy to be more than 96 percent against any grade of cervical, vulvar and vaginal disease and more than 93 percent efficacy against six-month persistent HPV infection.[67]
Studies in males, including men who have sex with men, have shown that HPV4 vaccine is efficacious against anal HPV infection and associated precancerous lesions.[9, 68,69] HPV4 protects men vaccinated between ages 16–26 years against genital warts or external genital lesions compared with unvaccinated dummy controls.[45]
Effectiveness
A 2016 systematic review of published literature summarised the global experiences with HPV4 from 1 January 2007 to 29 February 2016.[70] It assessed the global effect of HPV4 vaccine on HPV infection, genital warts and cervical abnormalities based on 57 publications across nine countries. The greatest impact was seen in countries with high vaccine uptake and among girls vaccinated prior to HPV exposure. Maximal reductions of around 90 percent were reported for vaccine-type HPV infections (6, 11, 16, 18) and genital wart cases.
For women vaccinated before the age of 20 years, the risk of CIN2+ was significantly lower than in unvaccinated women (effectiveness of at least one dose is 58–77 percent).[71,72,73]
Duration of protection
As vaccination programmes have only been in place for little over a decade, the duration of protection is not yet fully known. Follow-up studies 8–10 years after HPV vaccination have shown no waning of protection.[1] Long-term studies are ongoing to determine the duration of efficacy for all HPV vaccines.
Herd immunity and population impact
In January 2019, WHO began considering a global strategy to eliminate cervical cancer and established clear targets to 2030. This is only achievable with high vaccination coverage and access to regular screening for all women.[74, 75]
Australia saw a reduction in the prevalence of vaccine-type HPV infections (6, 11, 16, 18) in unvaccinated young men after the introduction of the vaccine to young women, supporting the role of herd immunity.[76,77,78] There was also a significant decrease in the prevalence of vaccine-type HPV infections in unvaccinated women (aged 25 years or younger).[79] Vaccination of females has provided herd immunity against oropharyngeal HPV16 prevalence in unvaccinated males in the UK.[80]
In a study of sexual health clinic data in Melbourne, the researchers noted the near disappearance of genital warts in women and heterosexual men aged under 21 years.[78] In addition, the data indicated that the basic reproductive rate (see section 1.2.1) had fallen below one. This reduction in cases occurred without any corresponding reduction in women aged over 30 years, men who have sex with men and non-residents. Similar trends were noted in the data from the Australian genital warts national surveillance network.
Eleven years after the introduction of HPV4 vaccine in the US, HPV4 types declined by 81 percent in vaccinated women and 40 percent in unvaccinated women. As well as direct protection from HPV9 vaccine, potential cross-protection from HPV4 was also observed in vaccinated women with a 71 percent decline in prevalence of the additional, genetically related HPV9 types.[4]
Previous exposure to HPV
While efficacy is unclear, there are no safety concerns in offering vaccination to women who have had HPV-related disease and would like to use the vaccine to reduce the risk of further disease.
A retrospective analysis of the HPV4 vaccine’s pivotal efficacy trial data (Future I and Future II) studied a group of women who were vaccinated before they had their first treatment for HPV-related disease.[81] This showed a reduction in subsequent HPV‑related disease in vaccinated women aged 15–26 years who had received treatment for cervical, vulvar or vaginal disease during the trial. The study showed a 46.2 percent reduction (95% CI: 22.5–63.2) after cervical surgery of any HPV-related disease and 35.2 percent reduction (95% CI: 18.8–51.8) after diagnosis of genital warts or vaginal or vulvar disease.
In contrast, a systematic review found that there was no evidence that HPV vaccines were effective in preventing vaccine-type HPV-associated precancer in pre-exposed women. This review explored efficacy against CIN3+ precancers in women with evidence of prior vaccine-type HPV exposure in three randomised controlled trials and two post-trial cohort studies.[82] Despite these findings, it was concluded that longer-term benefits in preventing re-infection could not be excluded (ie, the vaccine is not therapeutic but may prevent future infection, emphasising the importance of vaccination prior to sexual debut).
10.4.3. Transport, storage and handling
10.4.3. Transport, storage and handling
Transport according to the National Standards for Vaccine Storage and Transportation for Immunisation Providers 2017 (2nd edition).
Store in the dark at +2°C to +8°C. Do not freeze.
10.4.4. Dosage and administration
10.4.4. Dosage and administration
The dose of HPV vaccine is 0.5 mL, administered by intramuscular injection in the deltoid area (see section 2.2.3).
Co-administration with other vaccines
HPV vaccine may be co-administered with any live or inactivated vaccine indicated at the same visit.[1]
Interchangeability
All HPV vaccines may be used interchangeably for completion of a course.[83]
10.5. Recommended immunisation schedule
Table 10.3: HPV vaccine recommendations and schedules
Table 10.3: HPV vaccine recommendations and schedules
Note: HPV vaccine may be offered from age 9 years, but the usual Schedule will be at age 11/12 years (school years 7/8). Funded individuals are in shaded rows. See the Pharmaceutical Schedule (external link) for any changes to the funding decisions.
|
Recommended and funded |
Doses |
HPV Schedulea |
|---|---|---|
|
Children aged 14 years and undera |
2a |
0 and 6–12a months |
|
Individuals aged 15–26 yearsa,b |
3 |
0, 2 and 6 monthsc |
|
Individuals aged 9–26 years: |
|
|
|
3 |
0, 2 and 6 months |
|
||
|
An additional dose |
At least 1 month after the last dose of chemotherapy |
|
Recommended but not funded |
Doses |
HPV Schedule |
|
Individuals aged 27 years and older:a,b,e
|
3 |
0, 2 and 6 monthse |
|
a. See note in text for two-dose schedules, age groups and continuation of courses. b. The decision to vaccinate older age groups should follow an assessment of the potential benefits of vaccination – based on their likely previous HPV exposure and future risks. c. If a shortened schedule is required, the three doses can be given with a minimum of 4 weeks between doses one and two, and the third dose given at least 12 weeks after dose two. d. For more information see sections 4.3.9 and 4.3.10. e. HPV vaccines are approved for use in females and males aged 9–45 years. |
||
10.5.1. Recommended and funded
10.5.1. Recommended and funded
From 1 January 2017 males and females aged 26 years and under became eligible for HPV vaccine. Including males in a routine vaccination programme is expected to increase the benefit to the population in terms of reduction for both HPV-related cancer outcomes and genital warts.
Immunisation should preferably be completed before the onset of sexual activity. The optimal time for HPV administration is at age 9–13 years, as the immunogenicity is more effective when given younger and as most males and females in this age group would be naïve to all HPV types. However, individuals who have begun sexual activity may still benefit from vaccination. The decision to vaccinate older age groups should follow an assessment of the potential benefits of vaccination – based on their likely previous HPV exposure and future risks.
See Table 10.3 for HPV vaccine recommendations and schedules. A two-dose schedule of HPV at 0 and 6–12 months is recommended for individuals who receive the first dose before their 15th birthday, even if they are 15 years or older at the time of the second dose. Three doses are required for this age group if they have confirmed HIV infection or are transplant or chemotherapy patients, or if the minimum dosing interval is not met (see below). Older individuals from age 15 years receive three doses of HPV vaccine, at 0, 2 and 6 months.
Note
For the two-dose HPV schedule for children aged 14 years and under:
- a two-dose schedule at least 6–12 months apart is recommended for individuals who receive the first dose before their 15th birthday, even if they are 15 years or older at the time of the second dose
- the second dose is preferably given at least 6–12 months after the first; if the second dose is given less than five months after the first, a third HPV dose is recommended and funded – give the third HPV dose at least five months after the first.
Individuals who started with HPV4 may complete their remaining doses with HPV9.
Individuals who were fully vaccinated with HPV4 do not require further vaccination with HPV9. Any further protection is likely to be limited, particularly, if they have already been exposed through sexual contact. Most HPV-associated cancers result from infection with HPV types 16 and 18, which are covered by HPV4 (see Table 10.1).
Individuals who were under age 27 years when they commenced HPV vaccination are currently funded to complete the three-dose course, even if they are older than 27 years when they complete it.
Non-residents who were under age 18 years when they commenced HPV vaccination are currently funded to complete the course, even if they are older than 18 years when they complete it.
10.5.2. Recommended but not funded
10.5.2. Recommended but not funded
Individuals aged 27 years and older
The decision to vaccinate older age groups should follow an assessment of the potential benefits of vaccination – based on their likely previous HPV exposure and future risks. HPV9 is approved for use in females and males aged 9–45 years.
The data from the pivotal studies for HPV4 has demonstrated potential benefit to some women older than 25 years and the vaccine was shown to be effective at preventing infection and disease from the vaccine types in women aged 24–45 years who were uninfected at baseline.[84] However, pre-vaccination testing for cervical cytological abnormalities or for HPV infection is not recommended.
10.5.3. Pregnancy and breastfeeding
10.5.3. Pregnancy and breastfeeding
HPV vaccines are not recommended for pregnant women; however, enquiring about the possibility of pregnancy is not necessary before vaccination.[85]
Data to date shows no adverse effects of HPV vaccines on pregnancy outcomes.[1, 86, 87] However, if a vaccine dose has been administered around the time of conception or during pregnancy, health professionals are advised to report this to CARM (see section 1.6.3) and the vaccine manufacturer to assist with ongoing safety monitoring. If a woman is found to be pregnant after starting the HPV vaccine schedule, the remaining doses should be delayed until after pregnancy.
HPV vaccines may be given to breastfeeding women.[88]
10.6. Contraindications and precautions
See section 2.1.3 for pre-vaccination screening guidelines and section 2.1.4 for general contraindications for all vaccines.
10.6.1. Contraindications
10.6.1. Contraindications
HPV vaccine should not be administered to people with a history of an anaphylactic reaction to a prior dose of HPV vaccine or to a vaccine component. HPV vaccines contain HPV proteins produced by genetically engineered yeast cells. They should not, therefore, be given to people with a history of an immediate hypersensitivity to yeast.
10.6.2. Precautions
10.6.2. Precautions
Pregnancy is a precaution – see section 10.5.3.
10.7. Potential responses and AEFIs
HPV vaccines have excellent safety profiles internationally. There have been no safety signals raised since the vaccines were licensed, and a number of large investigations have been carried out to assess specific outcomes, particularly autoimmune conditions.[89, 90, 91, 92, 93] Post‑marketing surveillance systems globally continue to monitor the safety of HPV vaccination programmes.[94, 95, 96] The WHO’s Global Advisory Committee on Vaccine Safety has systematically reviewed HPV vaccine safety and has not found any safety issue that would alter its recommendations for use.[97, 98] The main challenge with HPV vaccine is communicating its excellent safety profile.[99] (See also the HPV discussion in section 3.2.4.)
Syncope (fainting) occurs frequently in adolescents following vaccination, but this is a stress response to being vaccinated, not a reaction to the vaccine.[2, 100, 101] WHO recognises immunisation-related stress responses as potential responses to HPV vaccination (see section 2.3.3).[102]
Safety has been evaluated in approximately 15,000 subjects in the HPV9 clinical development programme and no new safety signals have been shown through post-marketing surveillance.[83, 103] The vaccine is well-tolerated, and most adverse events were injection-site-related pain, swelling, and erythema that were mild to moderate in intensity. The safety profile of HPV9 is like HPV4. Female HPV9 recipients had more injection-site adverse events than female HPV4 recipients, including swelling (40.3 percent compared to 29.1 percent in HPV4 recipients) and erythema (34 percent compared to 25.8 percent in HPV4 recipients). Male recipients had fewer injection-site adverse events and were similar following either vaccine. Rates of injection-site swelling and erythema both increased following each successive dose of HPV9.
In summary, HPV9 is well-tolerated in all age groups, although it is slightly more reactogenic than HPV4.[59, 61, 83] The most common adverse events are pain, swelling, erythema, pruritus, headache and pyrexia. The frequency of these common adverse events is increased slightly (up to two-fold) when concurrent vaccinations are given.[104]
10.8. Cancer prevention measures
For women, HPV immunisation is part of a three-pronged approach to cervical cancer prevention that also includes regular cervical screening and safer sex approaches. For men, HPV immunisation and safer sex approaches are expected to contribute to the prevention of HPV-related cancers and disease that affect men, as well as cervical cancer prevention in women.
10.8.1. HPV immunisation
10.8.1. HPV immunisation
By preventing infection with oncogenic HPV types, HPV vaccination can reduce the incidence of precursor lesions that may lead to cancer. Vaccination needs to be administered before HPV infection occurs to prevent atypia and malignancy. Because genital HPVs are so common and so readily transmitted, in practical terms vaccination should be offered before the onset of sexual activity; that is, during or prior to early adolescence.
HPV immunisation does not reduce the progression of established disease but can be used in therapeutic situations by preventing the reactivation of latent infection or acquiring new infections.
10.8.2. Regular cervical screening for women
10.8.2. Regular cervical screening for women
A successful HPV immunisation programme for men and women will reduce the community prevalence of HPV infection and thus the incidence of cervical cancer in women. However, HPV immunisation alone will not completely eliminate cervical cancer, because some women will not have been vaccinated, a few will not develop immunity despite vaccination, and some will be infected prior to vaccination or with oncogenic types not included in the vaccine.
Consequently, women will need to continue to undergo regular cervical screening to detect those precancerous lesions that occur despite vaccination. Cervical screening programmes are based on regular cytological screening or HPV testing to detect, monitor and treat at an early-stage precancerous lesion, or CIN. These programmes have been successful in reducing invasive disease and mortality.
Although the frequency of abnormal cytology is lower in the vaccinated group, women who have received HPV immunisation should still take part in the National Cervical Screening Programme. Three-yearly cervical smears are recommended for women between the ages of 25 and 70 years who have ever been sexually active.
10.8.3. Safer sex approaches
10.8.3. Safer sex approaches
To minimise the risk of HPV infection (plus other sexually transmitted infections), practitioners should remind individuals of safer sex approaches, including sexual abstinence, monogamous relationships, delayed sexual debut and minimising the number of sexual partners.[1] Consistent and correct use of condoms can decrease the risk of anogenital HPV infection when infected areas are covered or protected by the condom. However, HPV transmission in the genital region may occur even when condoms are used and does not necessarily require penetrative intercourse.[8]
10.9. Variations from the vaccine data sheets
For the three-dose schedules, the HPV vaccine data sheets recommend that all three doses are given within a 12-month period. Health New Zealand recommends that if the three-dose schedule has been interrupted, prior doses do not need to be repeated regardless of how long ago the previous doses were given (see Appendix 2).
The HPV9 data sheet states that there are no studies on the interchangeability of HPV vaccines. Health New Zealand recommends that all HPV vaccines may be used interchangeably for completion of a course.[83] Those individuals who started with HPV4 may complete their remaining doses with HPV9.
References
References
References
- American Academy of Pediatrics. 2018. Human papillomaviruses. in Red Book: 2018 Report of the Committee on Infectious Diseases, Kimberlin D, Brady M, Jackson M, et al. (eds). URL: https://redbook.solutions.aap.org/redbook.aspx (external link). (accessed 3 July 2020)
- Schiller JT, Markowitz LE, Hildesheim A, et al. 2018. Human papillomavirus vaccines, in Plotkin's Vaccines (7th edition), Plotkin S, Orenstein W, Offit P, et al. (eds). Elsevier: Philadelphia, US.
- Saraiya M, Unger ER, Thompson TD, et al. US assessment of HPV types in cancers: implications for current and 9-valent HPV vaccines. Journal of the National Cancer Institute, 2015. 107(6): p. djv086.
- Spinner C, Ding L, Bernstein DI, et al. Human Papillomavirus Vaccine Effectiveness and Herd Protection in Young Women. Pediatrics, 2019. 143(2).
- Ministry of Health. 2007. High Grade Squamous Intra-epithelial Lesions (HSIL) in New Zealand (ed.), Wellington: Ministry of Health, National Cervical Screening Programme, National Screening Unit. URL: https://www.nsu.govt.nz/system/files/resources/hsil-in-new-zealand.pdf (external link) (accessed 3 July 2020)
- McFadden K, McConnell D, Salmond C, et al. Socioeconomic deprivation and the incidence of cervical cancer in New Zealand: 1988–1998. New Zealand Medical Journal, 2004. 117(1206): p. U1172.
- Partridge JM, Hughes JP, Feng Q, et al. Genital human papillomavirus infection in men: incidence and risk factors in a cohort of university students. Journal of Infectious Diseases, 2007. 196(8): p. 1128-36.
- Winer RL, Lee SK, Hughes JP, et al. Genital human papillomavirus infection: incidence and risk factors in a cohort of female university students. American Journal of Epidemiology, 2003. 157(3): p. 218-26.
- Giuliano AR, Palefsky JM, Goldstone S, et al. Efficacy of quadrivalent HPV vaccine against HPV Infection and disease in males. New England Journal of Medicine, 2011. 364(5): p. 401-11.
- Centers for Disease Control and Prevention. 2012. Human papillomavirus-associated cancers – United States, 2004–2008. Morbidity and Mortality Weekly Report. 61(15): p. 258–61. URL: www.cdc.gov/mmwr/preview/mmwrhtml/mm6115a2.htm (accessed 3 July 2020)
- Smith JS, Gilbert PA, Melendy A, et al. Age-specific prevalence of human papillomavirus infection in males: a global review. Journal of Adolescent Health, 2011. 48(6): p. 540-52.
- Machalek DA, Poynten M, Jin F, et al. Anal human papillomavirus infection and associated neoplastic lesions in men who have sex with men: a systematic review and meta-analysis. Lancet Oncology, 2012. 13(5): p. 487-500.
- Zou H, Tabrizi SN, Grulich AE, et al. Early acquisition of anogenital human papillomavirus among teenage men who have sex with men. Journal of Infectious Diseases, 2014. 209(5): p. 642-51.
- Vajdic CM, van Leeuwen MT, Jin F, et al. Anal human papillomavirus genotype diversity and co-infection in a community-based sample of homosexual men. Sexually Transmitted Infections, 2009. 85(5): p. 330-5.
- Grulich AE, van Leeuwen MT, Falster MO, et al. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: a meta-analysis. Lancet, 2007. 370(9581): p. 59-67.
- Wilkin T, Lee JY, Lensing SY, et al. Safety and immunogenicity of the quadrivalent human papillomavirus vaccine in HIV-1-infected men. Journal of Infectious Diseases, 2010. 202(8): p. 1246-53.
- Beachler DC, Weber KM, Margolick JB, et al. Risk factors for oral HPV infection among a high prevalence population of HIV-positive and at-risk HIV-negative adults. Cancer Epidemiology, Biomarkers and Prevention, 2012. 21(1): p. 122-33.
- Begue R. Immunization recommendations for the HIV-infected adolescent. HIV Clinician, 2012. 24(2): p. 15-21.
- Panel on Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV. Human papillomavirus disease. in Guidelines for the Prevention and Treatment of Opportunistic Infections in HIV-infected Adults and Adolescents: Recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. URL: https://aidsinfo.nih.gov/contentfiles/lvguidelines/adult_oi.pdf (external link). (accessed 3 July 2020)
- de Sanjose S, Quint WG, Alemany L, et al. Human papillomavirus genotype attribution in invasive cervical cancer: a retrospective cross-sectional worldwide study. Lancet Oncology, 2010. 11(11): p. 1048-56.
- Sarian LO, Derchain SF, Pitta Dda R, et al. Factors associated with HPV persistence after treatment for high-grade cervical intra-epithelial neoplasia with large loop excision of the transformation zone (LLETZ). Journal of Clinical Virology, 2004. 31(4): p. 270-4.
- Safaeian M, Hildesheim A, Gonzalez P, et al. Single nucleotide polymorphisms in the PRDX3 and RPS19 and risk of HPV persistence and cervical precancer/cancer. PloS One, 2012. 7(4): p. e33619.
- Syrjanen S. The role of human papillomavirus infection in head and neck cancers. Annals of Oncology, 2010. 21 Suppl 7(Suppl 7): p. vii243-5.
- Plummer M, de Martel C, Vignat J, et al. Global burden of cancers attributable to infections in 2012: a synthetic analysis. Lancet Glob Health, 2016. 4(9): p. e609-16.
- de Martel C, Plummer M, Vignat J, et al. Worldwide burden of cancer attributable to HPV by site, country and HPV type. International Journal of Cancer, 2017. 141(4): p. 664-670.
- Winer RL, Feng Q, Hughes JP, et al. Risk of female human papillomavirus acquisition associated with first male sex partner. Journal of Infectious Diseases, 2008. 197(2): p. 279-82.
- Bruni L, Albero G, Serrano B, et al. 2019. Human Papillomavirus and Related Diseases in the World. Summary Report (ed.), Barcelona, Spain: ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). URL: https://hpvcentre.net/statistics/reports/XWX.pdf (external link) (accessed 12 March 2020)
- Kjaer SK, Frederiksen K, Munk C, et al. Long-term absolute risk of cervical intraepithelial neoplasia grade 3 or worse following human papillomavirus infection: role of persistence. Journal of the National Cancer Institute, 2010. 102(19): p. 1478-88.
- Mallen-St Clair J, Alani M, Wang MB, et al. Human papillomavirus in oropharyngeal cancer: The changing face of a disease. Biochimica et Biophysica Acta, 2016. 1866(2): p. 141-150.
- Wiley DJ, Douglas J, Beutner K, et al. External genital warts: diagnosis, treatment, and prevention. Clinical Infectious Diseases, 2002. 35(Suppl 2): p. S210-24.
- Koutsky L. Epidemiology of genital human papillomavirus infection. American Journal of Medicine, 1997. 102(5A): p. 3-8.
- Kjaer SK, Tran TN, Sparen P, et al. The burden of genital warts: a study of nearly 70,000 women from the general female population in the 4 Nordic countries. Journal of Infectious Diseases, 2007. 196(10): p. 1447-54.
- Clark TC, Fleming T, Bullen P, et al. 2013. Youth’12 Overview: The health and wellbeing of New Zealand secondary school students in 2012 (ed.), Auckland, New Zealand: The University of Auckland. URL: https://www.fmhs.auckland.ac.nz/assets/fmhs/faculty/ahrg/docs/2012-overview.pdf (external link) (accessed 13 March 2020)
- Clark TC, Fleming T, Bullen P, et al. 2013. Youth’12 Prevalence Tables: The health and wellbeing of New Zealand secondary school students in 2012 (ed.), Auckland, New Zealand: The University of Auckland. URL: https://www.fmhs.auckland.ac.nz/assets/fmhs/faculty/ahrg/docs/2012prevalence-tables-report.pdf (external link) (accessed 13 March 2020)
- Clark TC, Lucassen MF, Fleming T, et al. Changes in the sexual health behaviours of New Zealand secondary school students, 2001-2012: findings from a national survey series. Australian and New Zealand Journal of Public Health, 2016. 40(4): p. 329-36.
- Kang YJ, Lewis H, Smith MA, et al. Pre-vaccination type-specific HPV prevalence in confirmed cervical high grade lesions in the Maori and non-Maori populations in New Zealand. BMC Infectious Diseases, 2015. 15(365): p. 365.
- Simonella LM, Lewis H, Smith M, et al. Type-specific oncogenic human papillomavirus infection in high grade cervical disease in New Zealand. BMC Infectious Diseases, 2013. 13: p. 114.
- Sykes P, Gopala K, Tan AL, et al. Type distribution of human papillomavirus among adult women diagnosed with invasive cervical cancer (stage 1b or higher) in New Zealand. BMC Infectious Diseases, 2014. 14: p. 374.
- Ministry of Health. 2019. Selected Cancers 2015, 2016, 2017 (ed.): Ministry of Health. URL: https://www.health.govt.nz/publication/selected-cancers-2015-2016-2017 (external link) (accessed 13 March 2020)
- Ministry of Health. 2016 Mortality 2014 data tables. 2016; URL: https://www.health.govt.nz/publication/mortality-2014-data-tables (external link). (accessed 3 July 2020)
- Chelimo C ,Elwood JM. Sociodemographic differences in the incidence of oropharyngeal and oral cavity squamous cell cancers in New Zealand. Australian and New Zealand Journal of Public Health, 2015. 39(2): p. 162-7.
- Lucas-Roxburgh R, Benschop J, Lockett B, et al. The prevalence of human papillomavirus in oropharyngeal cancer in a New Zealand population. PloS One, 2017. 12(10): p. e0186424.
- Wilson N, Morgan J ,Baker MG. Evidence for effectiveness of a national HPV vaccination programme: national prescription data from New Zealand. Sexually Transmitted Infections, 2014. 90(2): p. 103.
- Oliphant J, Stewart J, Saxton P, et al. Trends in genital warts diagnoses in New Zealand five years following the quadrivalent human papillomavirus vaccine introduction. New Zealand Medical Journal, 2017. 130: p. 1452.
- Bergman H, Buckley BS, Villanueva G, et al. Comparison of different human papillomavirus (HPV) vaccine types and dose schedules for prevention of HPV-related disease in females and males. Cochrane Database Syst Rev, 2019. 2019(11).
- Donken R, Knol MJ, Bogaards JA, et al. Inconclusive evidence for non-inferior immunogenicity of two- compared with three-dose HPV immunization schedules in preadolescent girls: A systematic review and meta-analysis. Journal of Infection, 2015. 71(1): p. 61-73.
- Sankaranarayanan R, Prabhu PR, Pawlita M, et al. Immunogenicity and HPV infection after one, two, and three doses of quadrivalent HPV vaccine in girls in India: a multicentre prospective cohort study. Lancet Oncology, 2016. 17(1): p. 67-77.
- D'Addario M, Redmond S, Scott P, et al. Two-dose schedules for human papillomavirus vaccine: Systematic review and meta-analysis. Vaccine, 2017. 35(22): p. 2892-2901.
- Joura EA, Kjaer SK, Wheeler CM, et al. HPV antibody levels and clinical efficacy following administration of a prophylactic quadrivalent HPV vaccine. Vaccine, 2008. 26(52): p. 6844-51.
- Einstein MH, Baron M, Levin MJ, et al. Comparison of the immunogenicity and safety of Cervarix and Gardasil human papillomavirus (HPV) cervical cancer vaccines in healthy women aged 18-45 years. Hum Vaccin, 2009. 5(10): p. 705-19.
- Rowhani-Rahbar A, Alvarez FB, Bryan JT, et al. Evidence of immune memory 8.5 years following administration of a prophylactic human papillomavirus type 16 vaccine. Journal of Clinical Virology, 2012. 53(3): p. 239-43.
- MacIntyre CR, Shaw P, Mackie FE, et al. Immunogenicity and persistence of immunity of a quadrivalent Human Papillomavirus (HPV) vaccine in immunocompromised children. Vaccine, 2016. 34(36): p. 4343-50.
- Gomez-Lobo V, Whyte T, Kaufman S, et al. Immunogenicity of a prophylactic quadrivalent human papillomavirus L1 virus-like particle vaccine in male and female adolescent transplant recipients. Pediatric Transplantation, 2014. 18(3): p. 310-5.
- Giacomet V, Penagini F, Trabattoni D, et al. Safety and immunogenicity of a quadrivalent human papillomavirus vaccine in HIV-infected and HIV-negative adolescents and young adults. Vaccine, 2014. 32(43): p. 5657-61.
- Kahn JA, Xu J, Kapogiannis BG, et al. Immunogenicity and safety of the human papillomavirus 6, 11, 16, 18 vaccine in HIV-infected young women. Clinical Infectious Diseases, 2013. 57(5): p. 735-44.
- Kojic EM, Kang M, Cespedes MS, et al. Immunogenicity and safety of the quadrivalent human papillomavirus vaccine in HIV-1-infected women. Clinical Infectious Diseases, 2014. 59(1): p. 127-35.
- Jacobson DL, Bousvaros A, Ashworth L, et al. Immunogenicity and tolerability to human papillomavirus-like particle vaccine in girls and young women with inflammatory bowel disease. Inflammatory Bowel Diseases, 2013. 19(7): p. 1441-9.
- Kumar D, Unger ER, Panicker G, et al. Immunogenicity of quadrivalent human papillomavirus vaccine in organ transplant recipients. American Journal of Transplantation, 2013. 13(9): p. 2411-7.
- Joura EA, Giuliano AR, Iversen OE, et al. A 9-valent HPV vaccine against infection and intraepithelial neoplasia in women. New England Journal of Medicine, 2015. 372(8): p. 711-23.
- Vesikari T, Brodszki N, van Damme P, et al. A randomized, double-blind, phase III study of the immunogenicity and safety of a 9-valent human papillomavirus L1 virus-like particle vaccine (V503) versus Gardasil® in 9-15-year-old girls. Pediatric Infectious Disease Journal, 2015. 34(9): p. 992-8.
- Castellsagué X, Giuliano AR, Goldstone S, et al. Immunogenicity and safety of the 9-valent HPV vaccine in men. Vaccine, 2015. 33(48): p. 6892-901.
- Van Damme P, Olsson SE, Block S, et al. Immunogenicity and Safety of a 9-Valent HPV Vaccine. Pediatrics, 2015. 136(1): p. e28-39.
- Seqirus/MSD. 2016 Gardasil 9 data sheet. URL: https://www.medsafe.govt.nz/profs/datasheet/g/gardasil9inj.pdf (external link). (accessed 10 May 2022)
- Xu L, Selk A, Garland SM, et al. Prophylactic vaccination against human papillomaviruses to prevent vulval and vaginal cancer and their precursors. Expert Rev Vaccines, 2019. 18(11): p. 1157-1166.
- Lehtinen M, Paavonen J, Wheeler CM, et al. Overall efficacy of HPV-16/18 AS04-adjuvanted vaccine against grade 3 or greater cervical intraepithelial neoplasia: 4-year end-of-study analysis of the randomised, double-blind PATRICIA trial. Lancet Oncology, 2012. 13(1): p. 89-99.
- Future II Study Group. Quadrivalent vaccine against human papillomavirus to prevent high-grade cervical lesions. New England Journal of Medicine, 2007. 356(19): p. 1915-27.
- Toh ZQ, Kosasih J, Russell FM, et al. Recombinant human papillomavirus nonavalent vaccine in the prevention of cancers caused by human papillomavirus. Infect Drug Resist, 2019. 12: p. 1951-1967.
- Palefsky JM, Giuliano AR, Goldstone S, et al. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. New England Journal of Medicine, 2011. 365(17): p. 1576-85.
- Swedish KA, Factor SH ,Goldstone SE. Prevention of recurrent high-grade anal neoplasia with quadrivalent human papillomavirus vaccination of men who have sex with men: a nonconcurrent cohort study. Clinical Infectious Diseases, 2012. 54(7): p. 891-8.
- Garland SM, Kjaer SK, Munoz N, et al. Impact and effectiveness of the quadrivalent human papillomavirus vaccine: a systematic review of 10 years of real-world experience. Clinical Infectious Diseases, 2016. 63(4): p. 519-27.
- Dehlendorff C, Sparen P, Baldur-Felskov B, et al. Effectiveness of varying number of doses and timing between doses of quadrivalent HPV vaccine against severe cervical lesions. Vaccine, 2018. 36(43): p. 6373-6378.
- Racey CS, Albert A, Donken R, et al. Cervical Intraepithelial Neoplasia Rates in British Columbia Women: A Population-Level Data Linkage Evaluation of the School-Based HPV Immunization Program. Journal of Infectious Diseases, 2020. 221(1): p. 81-90.
- Silverberg MJ, Leyden WA, Lam JO, et al. Effectiveness of catch-up human papillomavirus vaccination on incident cervical neoplasia in a US health-care setting: a population-based case-control study. Lancet Child Adolesc Health, 2018. 2(10): p. 707-714.
- Simms KT, Steinberg J, Caruana M, et al. Impact of scaled up human papillomavirus vaccination and cervical screening and the potential for global elimination of cervical cancer in 181 countries, 2020-99: a modelling study. Lancet Oncology, 2019. 20(3): p. 394-407.
- World Health Organization. 2020 Cervical cancer: Eliminating cervical cancer. 2020; URL: https://www.who.int/health-topics/cervical-cancer#tab=tab_2 (external link). (accessed 12 March 2020)
- Chow EPF, Machalek DA, Tabrizi SN, et al. Quadrivalent vaccine-targeted human papillomavirus genotypes in heterosexual men after the Australian female human papillomavirus vaccination programme: a retrospective observational study. Lancet Infectious Diseases, 2017. 17(1): p. 68-77.
- Donovan B, Franklin N, Guy R, et al. Quadrivalent human papillomavirus vaccination and trends in genital warts in Australia: analysis of national sentinel surveillance data. Lancet Infectious Diseases, 2011. 11(1): p. 39-44.
- Read TR, Hocking JS, Chen MY, et al. The near disappearance of genital warts in young women 4 years after commencing a national human papillomavirus (HPV) vaccination programme. Sexually Transmitted Infections, 2011. 87(7): p. 544-7.
- Chow EPF, Danielewski JA, Fehler G, et al. Human papillomavirus in young women with Chlamydia trachomatis infection 7 years after the Australian human papillomavirus vaccination programme: a cross-sectional study. The Lancet Infectious Diseases, 2015. 15(11): p. 1314-1323.
- Mehanna H, Bryant TS, Babrah J, et al. Human papillomavirus (HPV) vaccine effectiveness and potential herd immunity for reducing oncogenic oropharyngeal HPV-16 prevalence in the United Kingdom: A cross-sectional study. Clinical Infectious Diseases, 2019. 69(8): p. 1296-1302.
- Joura EA, Garland SM, Paavonen J, et al. Effect of the human papillomavirus (HPV) quadrivalent vaccine in a subgroup of women with cervical and vulvar disease: retrospective pooled analysis of trial data. BMJ, 2012. 344(e1401): p. e1401.
- Miltz A, Price H, Shahmanesh M, et al. Systematic review and meta-analysis of L1-VLP-based human papillomavirus vaccine efficacy against anogenital pre-cancer in women with evidence of prior HPV exposure. PloS One, 2014. 9(3): p. e90348.
- Petrosky E, Bocchini JA, Jr., Hariri S, et al. Use of 9-valent human papillomavirus (HPV) vaccine: updated HPV vaccination recommendations of the advisory committee on immunization practices. MMWR: Morbidity and Mortality Weekly Report, 2015. 64(11): p. 300-4.
- Muñoz N, Manalastas R, Jr., Pitisuttithum P, et al. Safety, immunogenicity, and efficacy of quadrivalent human papillomavirus (types 6, 11, 16, 18) recombinant vaccine in women aged 24-45 years: a randomised, double-blind trial. Lancet, 2009. 373(9679): p. 1949-57.
- Bonde U, Joergensen JS, Lamont RF, et al. Is HPV vaccination in pregnancy safe? Human Vaccines & Immunotherapeutics, 2016. 12(8): p. 1960-1964.
- Moreira ED, Jr., Block SL, Ferris D, et al. Safety Profile of the 9-Valent HPV Vaccine: A Combined Analysis of 7 Phase III Clinical Trials. Pediatrics, 2016. 138(2): p. e20154387.
- Wang A, Liu C, Wang Y, et al. Pregnancy outcomes after human papillomavirus vaccination in periconceptional period or during pregnancy: A systematic review and meta-analysis. Human Vaccines & Immunotherapeutics, 2019: p. 1-9.
- Australian Technical Advisory Group on Immunisation. 2018. Australian Immunisation Handbook (ed.), Canberra: Australian Government Department of Health. URL: https://immunisationhandbook.health.gov.au/ (external link) (accessed October 2019)
- Arnheim-Dahlstrom L, Pasternak B, Svanstrom H, et al. Autoimmune, neurological, and venous thromboembolic adverse events after immunisation of adolescent girls with quadrivalent human papillomavirus vaccine in Denmark and Sweden: cohort study. BMJ, 2013. 347: p. f5906.
- Chao C, Klein NP, Velicer CM, et al. Surveillance of autoimmune conditions following routine use of quadrivalent human papillomavirus vaccine. Journal of Internal Medicine, 2012. 271(2): p. 193-203.
- Grimaldi-Bensouda L, Guillemot D, Godeau B, et al. Autoimmune disorders and quadrivalent human papillomavirus vaccination of young female subjects. Journal of Internal Medicine, 2014. 275(4): p. 398-408.
- Langer-Gould A, Qian L, Tartof SY, et al. Vaccines and the risk of multiple sclerosis and other central nervous system demyelinating diseases. JAMA Neurol, 2014. 71(12): p. 1506-13.
- Scheller NM, Svanstrom H, Pasternak B, et al. Quadrivalent HPV vaccination and risk of multiple sclerosis and other demyelinating diseases of the central nervous system. JAMA, 2015. 313(1): p. 54-61.
- Gold MS ,McIntyre P. Human papillomavirus vaccine safety in Australia: experience to date and issues for surveillance. Sex Health, 2010. 7(3): p. 320-4.
- Kliewer EV, Demers AA, Brisson M, et al. The Manitoba human papillomavirus vaccine surveillance and evaluation system. Health Reports, 2010. 21(2): p. 37-42.
- Nguyen M, Ball R, Midthun K, et al. The Food and Drug Administration's Post-Licensure Rapid Immunization Safety Monitoring program: strengthening the federal vaccine safety enterprise. Pharmacoepidemiology and Drug Safety, 2012. 21 Suppl 1(Suppl 1): p. 291-7.
- World Health Organization. Global Advisory Committee on Vaccine Safety, 12–13 June 2013. Weekly Epidemiological Record, 2013. 88(29): p. 301–12.
- World Health Organization. Global Advisory Committee on Vaccine Safety, 4–5 December 2019 WEekly Epidemiological Record,, 2020. 95(4): p. 25-36.
- World Health Organization. Meeting of the Strategic Advisory Group of Experts on Immunization, April 2016 – conclusions and recommendations. Weekly Epidemiological Record 2016. 91(21): p. 266–84.
- Bonaldo G, Vaccheri A, D'Annibali O, et al. Safety profile of human papilloma virus vaccines: an analysis of the US Vaccine Adverse Event Reporting System from 2007 to 2017. British Journal of Clinical Pharmacology, 2019. 85(3): p. 634-643.
- Klein NP, Hansen J, Chao C, et al. Safety of quadrivalent human papillomavirus vaccine administered routinely to females. Archives of Pediatrics and Adolescent Medicine, 2012. 166(12): p. 1140-8.
- World Health Organization. 2019. Immunization Stress-related Response. A manual for program managers and health professionals to prevent, identify and respond to stress-related responses following immunization. (ed.), Geneva: World Health Organization. URL: https://www.who.int/publications-detail/978-92-4-151594-8 (external link) (accessed 07 May 2020)
- Donahue JG, Kieke BA, Lewis EM, et al. Near Real-Time Surveillance to Assess the Safety of the 9-Valent Human Papillomavirus Vaccine. Pediatrics, 2019. 144(6).
- Li Y, Zhu P, Wu M, et al. Immunogenicity and safety of human papillomavirus vaccine coadministered with other vaccines in individuals aged 9-25years: A systematic review and meta-analysis. Vaccine, 2020. 38(2): p. 119-134.