Pātiki and Waharua Kōpito patterns
On this page
Management of eating disorders
This pathway is for the primary care management of individuals, both male and female, with a suspected eating disorder up to the age of 18 or those in the final year of high school. It does not give any guidance around the secondary care management of these conditions.
Assessment
Assessment
Identification and screening
Early identification and treatment of patients with an eating disorder is hugely valuable and makes a real difference in the outcome. Patients in this group have the highest mortality of any psychiatric disorder.
- Eating disorders can be difficult to detect in primary care.
- They will often be identified in educational settings from the school nurse or a teacher or from parental concerns.
- Individuals are often presented by parents or caregivers rather than themselves.
- Routine psychological assessment is probably the best way to pick up an eating disorder, and this can be done via a quick HEEADSSS assessment (see screening tools box)
- Target groups for screening:
- young women with low BMI compared with the age norm
- patients consulting with weight concerns who are not overweight
- women with menstrual disturbances or amenorrhea
- patients with gastro-intestinal symptoms, e.g. constipation, bloating, reflux
- patients with physical signs of starvation or repeated vomiting
- children with poor growth
- young people with type 1 diabetes and poor treatment adherence
- patients that present with dental problems e.g. gingivitis or toothache, may raise concerns if vomiting repeatedly.
- Higher risk groups for anorexia:
- young people who diet (x5 with moderate dieting, x18 with severe dieting)
- overweight people who suddenly lose a lot of weight
- boys who are into extreme exercise or body building.
- Useful questions:
- "Does your weight affect the way you feel about yourself?"
- "Are you satisfied with your eating patterns?
- "What do you think about your current weight and shape?
- "Have you cut out any food groups recently?"
- "Have you ever had anorexia?"
- "Has anybody ever suspected you have an eating disorder?"
- "Have you ever vomited or used laxatives, diuretics or enemas for weight loss or weight control?"
- Use the SCOFF questionnaire to help clarify any suspicion of an eating disorder – this is not a diagnostic tool but a guide:
- Do you make yourself sick because you feel uncomfortably full?
- Do you worry you have lost control over how much you eat?
- Have you recently lost > 1 stone (6.3kg) in a three-month period?
- Do you believe yourself to be fat when others say you are too thin?
- Would you say that food dominates your life?
(One point should be given for every “yes” answer; a score of more than or equal to 2 indicates a likelihood of anorexia nervosa or bulimia nervosa)
Screening tools
- HEEADSSS - Home, Education/Employment, Eating, Activities, Drugs & Alcohol, Sexuality, Suicide/ Depression,Safety - click here for some great online resources for training in this (external link).
- SCOFF questionnaire (see above).
Definitions
The diagnosis of an eating disorder will generally be made within the MDT team at a secondary level. The diagnostic criteria are stated here for reference only and should not be used over and above any clinical suspicion or concern regarding an individual’s presentation.
- Anorexia Nervosa (DSM V)
- Restriction of energy intake resulting in a significantly low body weight, or a less than minimally expected weight (based on age, sex or developmental trajectory)
- Intense fear of gaining weight; or persistent behaviour that interferes with weight gain, despite low weight
- Disturbance in body image; or persistent lack of recognition of the seriousness of the current low body weight
Sub-types: Restricting type, binge-eating/purging type
- Bulimia nervosa (DSM V)
- Recurrent episodes of binge eating (this involves eating an excessive amount of food in a discrete period of time AND a sense of lack of control)
- Recurrent inappropriate compensatory behaviours to prevent weight gain, such as vomiting, laxatives, diuretics, fasting or excessive exercise
- Frequency of at least once per week for three months
- Self-evaluation unduly influenced by body shape and weight
- Absence of anorexia nervosa
Subtypes: Purging type, non-purging type
- Avoidant or restrictive food intake disorder (ARFID)
- Eating or feeding disturbance with persistent failure to meet nutritional needs associated with either significant weight loss (or growth failure), significant nutritional deficiency, dependence on enteral/supplemental feeding or marked interference with psychosocial functioning
- Not explained by lack of available food or culturally sanctioned practice
- Absence of anorexia nervosa, bulimia nervosa or body image disturbance
- No intercurrent medical illness:
-
-
- Avoidant Restrictive Food Intake Disorder (ARFID) is a new diagnostic category in the DSM-5. It is defined as a persistent feeding or eating disturbance leading to avoidance of food, which results in significant weight loss or nutritional deficiency and/or impairment in psychosocial functioning. Unlike anorexia nervosa and bulimia nervosa, ARFID is not characterised by preoccupation with body shape and weight or by intentional weight loss behaviours. Instead, patients suffering from ARFID may be disinterested in food and eating with lack of appetite leading to slower rate of eating, eating smaller portions, and greater struggles around food.
- It is quite important to distinguish ARFID from picky eating, which is relatively common among children (20-30%) but only for a small subgroup of picky eaters their behaviour becomes more persistent, leading to either malnutrition and weight loss with medical complications similar to anorexia nervosa and/or impairment of psychosocial functioning. The avoidance of eating may also be caused by traumatic experiences related to consuming food, such as a personal or witnessed episode of choking, gagging or vomiting.
- Common Signs of ARFID
- Long history of ‘picky eating’ since childhood
- Lack of interest in food and eating
- Lack of appetite
- Slow rate of eating
- Eating smaller portions
- Greater struggles around food
- Avoidance of foods because of dislike of colour, texture, smell or taste
- Fear of choking, gagging or vomiting
- Gastrointestinal complaints like bloating, heartburn, nausea, constipation
- Weight loss and signs of malnutrition
- Avoidance of situations of social eating
-
- Binge eating disorder
- Recurrent episodes of binge eating
- Associated with symptoms such as eating more rapidly, feeling uncomfortably full, not feeling hungry, eating alone due to embarrassment and/or feelings of self-disgust
- Marked distress regarding binge eating
- Frequency of at least once per week for three months
- Absence of compensatory behaviours, anorexia nervosa and bulimia nervosa
- Other specified FED (OSFED)
- Eating disorders causing significant distress but not meeting criteria for other diagnostic categories.Examples include:
- Atypical anorexia nervosa – ‘normal weight anorexia nervosa’
- Bulimia nervosa (of low frequency and/or limited duration)
- Subthreshold binge – eating disorder
- Purging disorder
- Night eating syndrome
- Eating disorders causing significant distress but not meeting criteria for other diagnostic categories.Examples include:
History
Naturally, history will be targeted to the concerns raised. Useful areas to explore include:
- changes in behaviour around food
- general functioning at home and school
- changes in family and other relationships
- weight loss or gain, patterns or trends in BMI
- menstruation patterns
- specific symptoms – cold sensitivity, sleep disturbances, fainting or dizzy spells, dental problems, digestive problems, vomiting blood
- consider medical causes of weight loss, e.g. coeliac disease (see differential diagnosis).
Physical examination
- Height, accurate weight, BMI and BMI centile and previous measurements – This link has some good graphs. (external link)
- Lying and standing heart rate and blood pressure
- Body temperature
- Peripheral circulation – capillary refill, peripheral cyanosis, peripheral and sacral oedema
- Pubertal status
- Signs of binging or purging – including roughness on knuckle of index finger (Russell’s sign), enlargement of the parotid glands and dental erosion
- Evidence of deliberate self-harm – cuts or scars on the arms, thighs or abdomen
Investigations to consider
These may be done at the initial assessment but are not always helpful to do on an ongoing routine basis unless there is a valid reason to do so.
- Full blood count and ESR
- Urea and electrolytes, creatinine, calcium, magnesium, phosphate, random blood glucose
- Luteinising hormone, follicle-stimulating hormone, oestradiol (or testosterone, if male)
For young people with more advanced eating disorders or severe weight loss, add:
- Serum bicarbonate and pH on venous gas analysis (metabolic alkalosis may indicate vomiting)
- Liver function tests
- Thyroid function tests
- ECG – essential if any symptoms or signs of cardiac compromise, e.g. bradycardia, electrolyte abnormality, if patient has a BMI below 15kg/m3
Risk assessment
Patients with an eating disorder have a high risk in terms of their own safety and health. They have the highest mortality of any psychiatric disorder.
The factors involved in the assessment of risk in people with eating disorders include:
- medical risk
- psychological risk
- insight or capacity and motivation.
If there is immediate concern for safety it may be appropriate to contact the crisis team.
- Phone EBOP: 0800 774 545 or during business hours on 07 306 0154
- Phone WBOP: 0800 800 508 or during business hours 07 579 8329
If the patient requires compulsory assessment then they will need the Mental Health Act 1992. If this is needed then contact the duty authorised officer using the 0800 numbers above and they will provide the necessary forms.
Differential-diagnosis
Keep in mind that eating disorders may co-exist with other disorders.
- Consider other causes of weight loss if appropriate, such as:
- malabsorption, e.g. coeliac disease, inflammatory bowel disease
- diabetes mellitus
- glandular fever
- cancer
- substance or stimulant misuse
- infection, e.g. tuberculosis
- autoimmune disease
- endocrine disorder – e.g. hypothyroidism, addison’s disease.
- Other causes of amenorrhea include:
- pregnancy
- primary ovarian failure
- polycystic ovarian syndrome
- pituitary prolactinoma
- hypothalamic cause.
- Psychiatric differential diagnoses include:
- depressive disorder or episode
- obsessive compulsive disorder
- psychotic disorder
- Pre-pubertal children may show symptoms of eating disorder secondary to:
- emotional and behavioural disorders
- phobias
- refusal disorder.
Management
Management
1. Red flags and criteria for possible admission
- Please see admission criteria below for guidance around who might need to be admitted.
- This table is for those patients who are acutely unwell when you are assessing them. Please see the referral for specialist assessment below for guidance on referring patients in for outpatient assessment.
- If you have any concerns about an individual with possible eating disorders then in the first instance please contact the paediatrician on-call at either Tauranga or Whakatane.
- It is important to note that those individuals who are admitted often have poorer outcomes and so careful assessment of the need for admission is vital.
Admission criteria
|
Life-threatening weight loss
|
Acute medical complications of malnutrition
|
|
Acute food refusal |
Significant dehydration |
|
Hypoglycaemia |
Electrolyte imbalance
|
|
Physiological Instability
|
Arrhythmia |
|
Significant co-morbid psychiatric states
|
Failure to gain weight despite maximum outpatient treatment |
- 2. Food challenge
If there is some uncertainly as to whether the individual has an eating disorder:
- express concern around stated symptoms or behaviour
- highlight possible physical/psychological consequences of continued concerning food related behaviours
- encourage healthy behaviour around food and weight, use online resources
- establish a weight goal – around 200-500mg/week
- set up follow up in 2-3 weeks
- 3. Review: 2-3 weeks
- At this visit – weigh and assess symptoms or behaviours
- If there has been weight gain, change in behaviour and insight is good then agree to further monitoring with monthly review and weight for next 3 months.
- If no ongoing concerns, nothing further.
4. If continued concerns, refer for specialist assessment
Referral for specialist assessment guidelines
- Refer into Paediatrics or MICAMHS for any concerns around weight loss with no obvious cause as well as any concerns regarding an eating disorder.
- Early intervention is associated with improved prognosis.
- The individual will have a joint MICAMHS/Paediatric assessment which will usually take place within a few weeks of receiving the referral.
- Please include all previous height or weight parameters and pulse in referral as well as the relevant history, other examination findings and investigation to date.
Resources
Resources
For patients and carers
- EDANZ
This is a New Zealand based website with a huge wealth of resources to help support and provide information for people with eating disorders and their families. - Maudsley Parents
This website offers information on eating disorders and family-based treatment, family stories of recovery, supportive parent-to-parent advice, and treatment information for families who opt for family-based Maudsley treatment. - Families Empowered and Supporting Treatment of Eating Disorders
- Infant, Child and Adolescent Mental Health
Information and support for families and friends.
For providers
- Early identification and treatment of patients with an eating disorder is hugely valuable and makes a real difference in outcome. Patients in this group have the highest mortality of any psychiatric disorder
- If you have any concerns about a patient with a possible eating disorder then please discuss these with a specialist. (external link)
- EDANZ
- Infant, Child and Adolescent Mental Health
- Eating Disorders Recognition and Treatment UK
Acknowledgments
Acknowledgments
This pathway was developed in collaboration with the following people:
- Dr Kendell Crossen - SMO Paediatrician/Adolescent Specialist
- Dr Alison James - GP Liaison
- Amber Fletcher - Clinical Psychologist/Eating Disorder Liaison
OST drug and drug related issues
Background
Background
The Tauranga Opioid Substitution Treatment service (OST) is one of the services offered by Bay of Plenty addiction services (BOPAS). It is part of the wider mental health and addiction service at Health New Zealand Bay of Plenty.
This pathway contains information and guidelines for general practitioners authorised by BOPAS OST to prescribe methadone or buprenorphine/naloxone to patients in the GP shared care programme. This information will assist in providing quality, safe, professionally delivered OST services that meets the needs of patients, their family, and the wider community. GPs and their staff are encouraged to consult with the addiction liaison clinician or the lead clinician at BOPAS OST working in a shared-care partnership model.
BOPAS OST provides services for the management of opioid dependency from a harm reduction philosophy, supporting people towards recovery, relative to each individual and his or her own circumstances.
The OST programme is in accordance with:
The BOPAS service manages the admission, stabilisation, and specialist maintenance phases of OST treatment. Patients may then be assessed as meeting criteria for the GP shared care programme where their OST is integrated with their primary health care provider who is authorised by BOPAS on a three-monthly (6-monthly with permission from the MOH) basis to prescribe methadone or buprenorphine/naloxone.
General drug issues
General drug issues
Increasing the Methadone or Buprenorphine/Naloxone dose
- This may be indicated when the patient is reporting that the dose is not sufficiently suppressing opioid withdrawal symptoms for the full 24 hours. The symptoms typically have their onset during the evening and overnight, are most marked in the hours before their usual dosing time and are markedly relieved within an hour or two of dose consumption. (See below, signs and symptoms of opioid withdrawal and intoxication or overdose).
- This may occur as the result of:
- ongoing development of tolerance to methadone or buprenorphine/naloxone.
- interaction with other medications or alcohol (see methadone or buprenorphine/naloxone interactions).
- decreased patient ability to manage previously tolerated mild withdrawal symptoms because of increased stress.
- cessation of illicit opioid use.
- Where continued, or relapse to illicit opioid use is reported:
- check for signs of injecting.
- check for signs of opioid intoxication.
- get a urinalysis done (full drug screen).
- enquire about triggers or stressors.
- Notes:
- Once a stable, comfortable dose has been achieved, it is not usual that the dose needs to be repeatedly adjusted upwards because of increasing tolerance.
- Patients may report craving without significant physical withdrawal. If in doubt, prescribers can defer a decision and advise patients to discuss with the Addiction Liaison Clinician.
- Measurement of serum levels may sometimes help inform a decision regarding dose adequacy. See serum levels page.
- In the situation of risky alcohol use (or other CNS depressants), methadone or buprenorphine/naloxone dose increase may actually increase clinical risk. Seek advice if necessary.
- Where, after careful clinical assessment, the decision is to trial an increase in dose, the G.P should contact the Addiction Liaison Clinician. Dose increases should be titrated up at no more than 5 to 10mgs at intervals of 5 to 7 days. It is advised to consider a temporary return to daily dispensing whilst re-stabilising, so that the pharmacist can also provide support and observe for any signs of sedation.
- If there is evidence of injecting, provide harm reduction information related to safer injecting practices and access to needle exchange. Notify Addiction Liaison Clinician.
- There are occasions when patients request an increase in dose to manage acute or chronic pain. We advise consultation with the Addiction Liaison Clinician before increasing the dose for pain relief. It is generally advised to add short-term additional medication for pain relief rather than altering OST medication.
Signs and symptoms of opioid withdrawal and intoxication or overdose
Signs and symptoms of opioid withdrawal:
- lacrimation
- perspiration
- fatigue
- yawning
- dilated pupils
- weakness
- restlessness
- gooseflesh
- abdominal cramps
- hot and cold flushes
- joint pain, backache
- drug seeking behaviour
- anorexia, nausea or diarrhoea
- muscle aches or leg cramps
- insomnia
- rhinorrhoea.
The onset of methadone or buprenorphine/naloxone withdrawal starts at 24 to 48 hours after the last dose. The duration of methadone or buprenorphine/naloxone withdrawal is up to 21 days. Psychological and neurological (including pain receptors) adjustments can last up to six months. Research indicates withdrawal symptoms from buprenorphine/naloxone are less than from methadone.
Signs and symptoms of opioid intoxication or overdose:
- sedation
- hypotension
- coma
- pulmonary oedema
- seizures
- scratching of skin
- respiratory depression
- pinpoint pupils
- bradycardia.
In cases of overdose ensure that the airway is clear and perform emergency cardiopulmonary resuscitation as necessary.
Transfer to hospital as soon as possible where treatment with an infusion of naloxone can be commenced.
Urine toxicology guidelines
- International evaluation of urinalysis shows that it is not in itself instrumental in reducing harm related to illicit drug use. Urinalysis provides information only about a patient's recent drug use and not about quantity, frequency or route of drug use and is a supplement to patient self-report. With these limitations in mind, urinalysis results are integrated into the clinical assessment.
- Research has consistently indicated that where patients do not have to be concerned that they will be punished for disclosure of illicit drug use the reliability of self-reported drug use increases.
- However, urinalysis may be indicated or useful in the following situations:
- where the patient or GP wishes to verify self-report of drug use
- where there is doubt regarding the accuracy of reported drug use or methadone or buprenorphine/naloxone consumption
- where the GP or pharmacist is concerned that a patient is intoxicated. Here a full drug screen is indicated
- as supportive information for monitoring by other services e.g. community corrections, child youth and family service
- for use in overall programme evaluation.
- Essential factors to promote reliability include:
- random sampling
- observed by medical officer or nurse
- requests must be on an appropriate laboratory request form.
- Note: If a patient does not complete a requested urinalysis further investigation is required.
- *See Appendix 6 Approximate Detection Time for Selected Drugs in Urine page 105 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
Serum levels
- Methadone serum levels are indicated when the clinical picture does not agree with expected/typical responses to a given dose of methadone and when this additional clinical information would be of use in making decisions regarding changes in the methadone dose.
- The serum methadone level for a given dose will vary between individuals because of individual tolerance and the influence of other factors (e.g. other medications, pregnancy, individual variations in hepatic metabolism and renal clearance).
- Research to date on the clinical application of serum methadone levels is inconsistent, generally indicating that the overall clinical picture must be the foundation for any decisions regarding adequacy of methadone dose. Serum levels may not provide conclusive information.
Consult with BOPAS OST prior to any serum level testing
Clinical situations where serum levels may be useful are:
- a client's responses to methadone OST does not align with the expected response
- a client is suspected of poor compliance with the programme, or of diverting their does (comparison of serum level measurements taken on the same individual within the last 6-12 months, with careful observation of dosing and retention of doses, may assist in determining compliance)
- when dose increase beyond 120mg/day is being considered (only to be done in conjunction with BOPAS).
- when there is doubt about the clinical indications for a dose increase
- if there is a suspected drug interaction
- when determining the need for split dosing (only to be done in conjunction with BOPAS)
- when there is doubt regarding the accuracy of reported methadone consumption-comparison of serum levels taken on the same individual within the last 6-12 months, may assist in determining compliance).
- in pregnancy
- when a client has a serious liver or other physical disease and there may be methadone accumulation.
Serum level testing
This procedure should be undertaken in liaison with the dispensing pharmacist and the BOPAS OST service.
- The patient must consume their methadone at the pharmacy at approximately the same time for 4 days (usually Monday to Thursday) prior to the blood test/s (on Friday). This is to ensure they reach a steady state for a known dose consumed daily under observation.
- On the day of the blood test the patient presents to the laboratory for their trough blood level to be taken before they consume their dose and at the same time, they have been consuming for previous four days.
- If clinically indicated (see split dosing) a peak blood level is taken 3 ½ to 4 hours after the patient has consumed their dose, and before any takeaway doses are dispensed.
- Serum methadone levels can be measured using capillary blood samples when venous access is difficult. A 1ml SST tube is sufficient.
Serum level interpretation and guidelines
- Serum methadone trough level: Level to provide 24-hour relief of withdrawal symptoms is usually 650-1000 ng/ml, though this should be approached on a case-by-case basis. Where a client presents with a higher trough level than 1000, this must be discussed with the OST specialist service.
- Serum methadone or buprenorphine/naloxone trough and peak levels:
- Where the peak: trough ratio is 2 or 2.5:1 or greater then split dosing may be indicated in a stable patient. Consult with the BOPAS OST Service, prior to instituting split dosing. See split methadone or buprenorphine/naloxone dosing.
- See Section 5.5 Measuring Methadone Serum Levels page 39 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
Treatment completion
- Entering and staying in treatment, coming off opioid substitution treatment and exiting structured treatment are all important indicators of an individual's recovery progress, but they do not in themselves constitute recovery. Coming off OST or exiting treatment prematurely can harm individuals, especially if it leads to relapse, which is also harmful to society. Recovery is broader and more complex journey that incorporates overcoming dependence, reducing risk-taking behaviour and offending, improving health, functioning as a productive member of society and becoming personally fulfilled. These recovery outcomes are often mutually reinforcing."The National Treatment Agency for Substance Misuse (2012) in the NZ Practice Guidelines for Opioid Substitution Treatment (2014) p26" (external link)
- Where a patient expresses an intention or desire to withdraw from methadone or buprenorphine/naloxone please contact the addiction liaison clinician for support with this.
- Consider:
- Motivation for withdrawal.
- Giving information to the patient e.g. the orange Coming off Methadone booklet.
- Discuss withdrawal options and develop a plan with the patient. BOPAS OST prefers clients are offered the opportunity to reduce "at request", so as to ensure they feel in control of their reduction regime at all times. For example, the script can be annotated to "reduce 1mg per week at request".
- Patients may also stop reduction for a period or have small dose increases before recommencing reductions. As with the opening quote; Recovery is broader and more complex journey.
- Review the withdrawal process each time the patient is seen or at the patient's request.
- Offer and negotiate a 'window period' of between 0 and 12 weeks with the patient during and prior to the completion of the withdrawal from methadone or buprenorphine/naloxone. The window period is the time after the last methadone or buprenorphine/naloxone dose is consumed within which the patient can choose to immediately re-stabilise on methadone or buprenorphine/naloxone. (Note: The restabilisation on methadone or buprenorphine/naloxone will be carried out by BOPAS OST, and the patient transferred back to the GP programme as appropriate).
- Notify the Addiction Liaison Clinician of the date on which the patient last consumed methadone or buprenorphine/naloxone and of the negotiated window period.
- If the patient makes contact wishing to re-stabilise on methadone or buprenorphine/naloxone within the window period contact the addiction liaison clinician about making an appointment at BOPAS OST for assessment regards re-stabilisation.
- If the patient makes contact wishing to recommence on methadone or buprenorphine/naloxone after the window period is completed then refer them to BOPAS for reassessment.
- If you believe that positive treatment outcomes will be compromised by withdrawal, contact the addiction liaison clinician to arrange a joint appointment with the patient to discuss and decide on an appropriate course of action, or contact the BOPAS OST, medical officer for advice and support.
Method of withdrawal
There is no ideal method of withdrawal from methadone or buprenorphine/naloxone. It is important that any reduction plan is done in consultation with the client, GP and addiction liaison clinician. Possible approaches to withdrawal are:
- Fixed: The rate of reduction of methadone or buprenorphine/naloxone is set by the GP in consultation with the patient and can only be altered by the GP. Recommended methadone reduction rate is 2.5mgs per script cycle. Some patients tolerate larger and faster initial reductions. Statistically the faster the reductions, the higher the rate of relapse as smaller reductions are better tolerated and momentum maintained.
- Flexible: The rate of reduction of methadone or buprenorphine/naloxone is entirely within the control of the client. The client and GP agree on a rate that is then added to the prescription, for example 1mg per week or 2mg per fortnight AT REQUEST. It then allows the client to access a reduction from the pharmacy whenever they feel ready. These patient-initiated dose changes may only be reductions, any increase in dose must be renegotiated with the GP and a new prescription written. The script must then be annotated with "adjust dose for reduction" to allow pharmacist to adjust the dose accordingly.
- Blind: The patient has the option of requesting a blind reduction, to be arranged by the GP in consultation with the addiction liaison clinician and pharmacist and the script to be appropriately annotated by the GP. The details of the dose reductions and administration are arranged by the GP with the pharmacist.
Decisions must be made after assessment of the patient's needs and preferences, and in consultation with the patient.
Rate of withdrawal recommended guidelines
| Current methadone or buprenorphine/naloxone dose/day | Weekly or fortnightly or monthly reduction |
|
Above 50mg |
5mg or less |
|
30-50mg |
2.5mg or less |
|
Less than 30mg |
1-2mg or less |
- The rate of withdrawal should be reviewed each time a patient is seen. If there is evidence that a patient's treatment outcomes are compromised by the rate of withdrawal, a slowing or cessation of the dose reduction, or even a temporary increase in the dose is recommended, rather than introducing ancillary medication.
- Note: Once down to 20mg per day or less, consider changing to the Biodone 2mg/ml substance to enable small reductions to be made more easily. The pharmacy will need to be notified in advance so that they can order this in.
- If clients struggle with the reduction off lower doses of methadone, they could be offered a transfer to Buprenorphine/naloxone, as this might be better tolerated.
- See Section 3.9.1 Planned Withdrawal page 29 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
Methadone specific issues
Methadone specific issues
Methadone specific issues
- Methadone is rapidly absorbed after oral administration with detectable plasma levels after 30 minutes.
- It undergoes considerable tissue distribution and crosses the blood brain barrier.
- Peak level is 3 to 4 hours after consumption.
- With regular doses the half-life is 6 to 96 hours with a mean of 25 hours.
- Steady state plasma levels are reached after approximately 4 hours.
- Methadone accumulates on repeated administration therefore doses should not be increased more often than every 4 days.
- *See Appendix 3 Pharmacology and Pharmacokinetics of Methadone and Buprenorphine page 97 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
Methadone toxicity
- Methadone causes respiratory depression and coma in overdose. There can be a narrow margin between a safe and a fatal dose especially in the presence of other CNS depressants (prescribed or illicit) or if there is no opioid tolerance established.
- For non-tolerant adults oral or parenteral doses of 50 mg or less have been fatal. Potentially fatal dose for children under 14 years is 10 mg.
- Potentially lethal overdoses can occur within 0.5 to 6 hours after ingestion by non-tolerant or partially tolerant individuals.
- A child consuming any quantity of methadone or buprenorphine/naloxone must be taken to an accident and emergency department immediately.
- This is one of the major underlying reasons behind the emphasis on safety and the limitations on takeaway doses in OST patients.
- *See Section 4.1 Overdose; 4.1.1 Consumption of takeaway doses by a child, page 30 of “New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
Metabolism and excretion
- Methadone is primarily metabolized in the liver and is excreted in urine and bile.
- A small amount is excreted unchanged by the kidneys and this amount increases with increased urinary acidity.
Methadone side effects
Some of these side effects may be confused with withdrawal symptoms and may be experienced even when the dose is appropriate.
| Side effects | Notes | Interventions/advice |
|---|---|---|
|
Aching muscles and joints |
Some individuals report rheumatic type pains and 'bone pain' - uncommon |
Medical examination for any underlying pathology. Hot Epsom salts bath may ease symptom |
|
Analgesia and hypo-analgesia |
Systemic analgesia, long term can lead to opiate receptor saturation and hypo-analgesia or increased pain sensation |
Advise patient to discuss chronic pain with GP/pain specialist |
|
Constipation |
A common side effect |
Increase intake of water and fiber and increase exercise. If necessary, take regular Lactulose or Movicol |
|
Galactorrhoea |
Due to mildly/moderately increased prolactin levels |
Check prolactin level and rule out pathology. Seek specialist endocrinologist advice if uncertain |
|
Irregular menstrual cycle/amenorrhoea |
Common in women who take opioids |
Educate women about the risk of pregnancy despite menstrual irregularity/amenorrhoea |
|
Lowered sex drive and impotence |
Common with all opioid use |
Reduce dose but needs to be weighed against compromising outcomes on MMT |
|
Oedema |
Fluid retention, puffiness, swelling, particularly of feet & ankles - uncommon |
Usually resolves within a few weeks of starting treatment |
|
Other G.I effects |
Include:
|
To reduce nausea and vomiting, suggest patient eat before consuming dose and drink dose slowly Other symptoms may be reduced by reducing the dose
|
|
Increased Perspiration |
Common especially at peak serum levels |
|
|
Q-T prolonging effect |
Potential for QTc prolongation, especially if combined with other drugs with similar effect |
Annual ECG tests recommended. See medications also with QT prolonging effects |
|
Sedation |
Drowsiness may be experience at peak serum level (3 to 4 hours after dose) especially during initial stabilisation |
Check serum levels Reduced dose or split dose may be necessary - see relevant sections |
|
Shallow breathing |
From the respiratory depressive action of opioids |
Reduce dose |
|
Skin rash/itching |
|
Appropriate skin lotion, e.g. BK lotion or similar emollient, antihistamine |
|
Tooth decay/dry mouth |
Opioids reduce the production of saliva |
|
|
Weight gain |
Occurs in small number of patients |
Assistance with weight management strategies |
|
Weight loss |
Lack of appetite, may be associated with mood |
Assistance with weight management strategies |
*See Section 6.2 Managing Side Effects page 44 and Appendix 4 Side Effects page 101 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
Interactions
- NZ Formulary (external link)
- *See Section 4.4 Drug Interactions page 34 and Appendix 5 Drug Interaction page 103 of New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)
How to write a prescription
Writing a methadone H572 controlled drug prescription
The use of H572M controlled drug prescription forms is restricted to prescribing methadone for patients under the authority conferred by Section 24(2) (d) Misuse of Drugs Act 1975 (i.e. where BOPAS has authorised a prescriber for a specific patient). The form is not used for prescribing of methadone to other patients in other circumstances (e.g. pain relief for a non-BOPAS client); in these cases the general H572 controlled drug prescription is used.
H572 prescription example
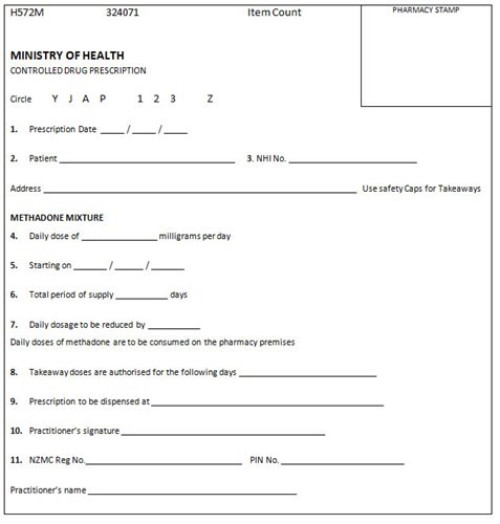
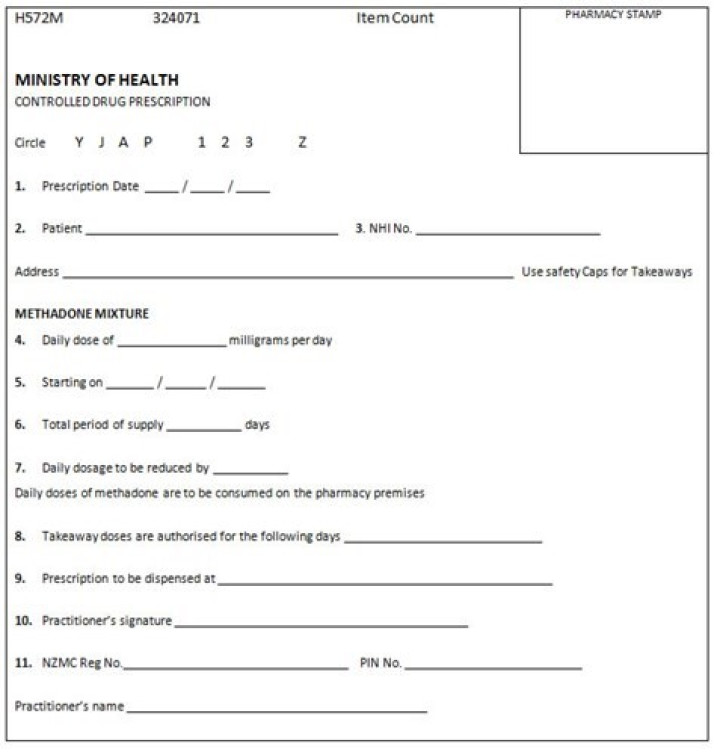
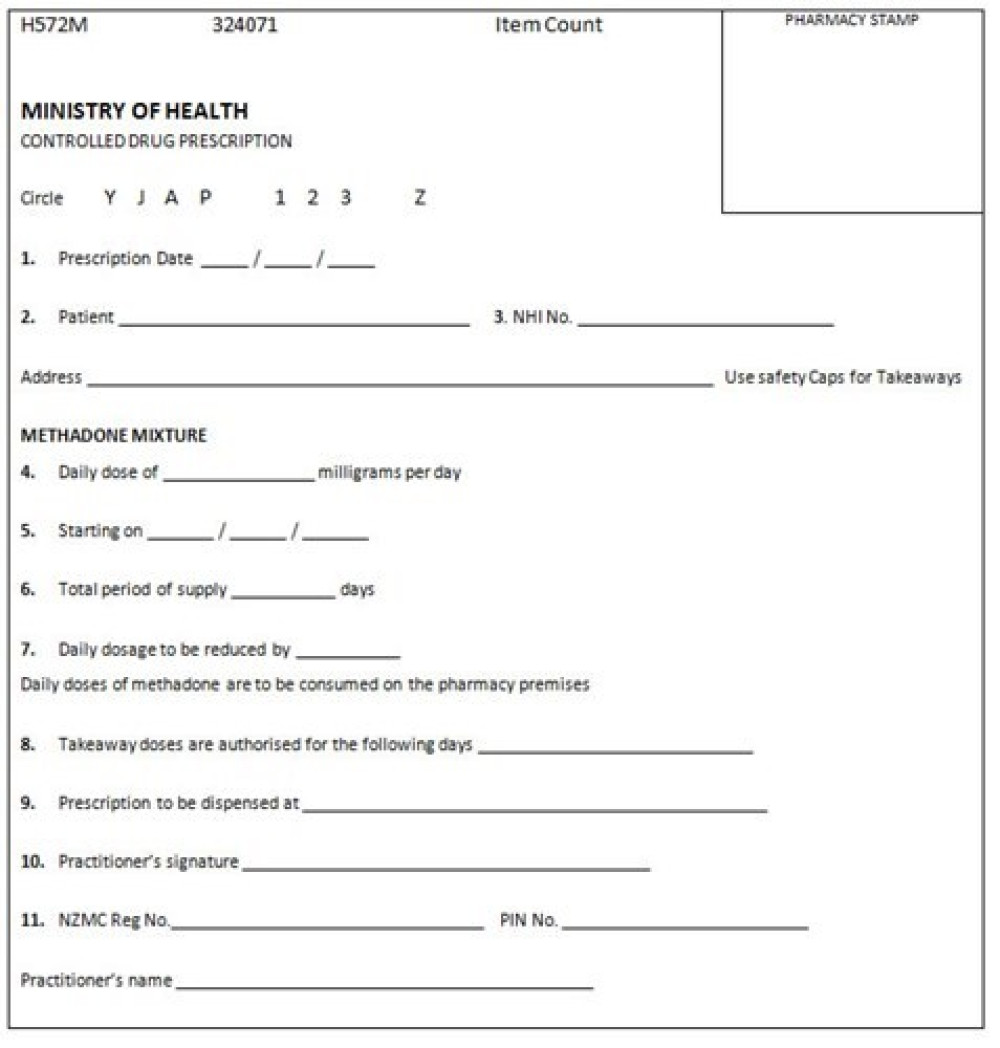
An example of a methadone H572 controlled drug prescription.
Instructions
- Date prescription written to be no more than 7 days from prescription starting date (point 5).
- Name and current residential address of patient. It is not acceptable to use the pharmacy address as the patient address.
- Patient's NHI number.
- Written dose, in numeric and word form e.g. 80 (eighty) mg. Note, if a patient is undertaking any type of withdrawal from methadone, then the new prescription should state the current dose as the starting dose. The script should then be annotated "adjust for reduction" to allow pharmacist to adjust the starting dose. Annotate with formulation of methadone to be used - BOPAS authorises 5mg/ml (consider isomg a stamp to pre-populate scripts). (2mg/ml can be used in doses under 20mg).
- Start date (actual date pharmacist is to begin dispensing). Check that the commencement date is a consumption day.
- Total period of supply up to a maximum of 30 days, however a 28-day cycle is routine to ensure ease of keeping to a regular cycle.
- Maximum rate of any withdrawal regimen (if any) is specified. eg. Reduce 1mg/week at request.
- Days for which takeaways are authorised. For example, 'Tuesday, Wednesday, Friday, Saturday and Sunday' for a patient on twice weekly dispensing who collects and consumes doses on Mondays and Thursdays.
- Name of pharmacy.
- Prescriber's signature.
- Prescriber's stamp or print NZMC Reg. No., doctor name and address. Each copy must be stamped.
- Top three copies to pharmacy (via patient or post). Note: Bottom copy (blue) to be kept on patient file; please do not send to the pharmacy.
Ordering
- These CD pads are requested 3-6 monthly by GPs based on their current number of authorised patients.
- Orders are faxed to the Ministry of Health using the approved order form (refer to Forms section). On receipt of the pads, sign the enclosed verification of delivery form and fax to the Ministry of Health as soon as possible.
Ministry of Health contacts
MedSafe Office
- phone: 09 441 3670
Storage
These CD pads must be stored in a secure place as for other CD prescription pads. You are advised to keep the receipt for the pads as a record of the prescription pad numbers.
Theft of prescription forms
If the prescription numbers are known, inform the Ministry of Health MedSafe office. If the prescription numbers are unknown, inform the Ministry of Health and request the prescription numbers of the pads recently sent to the practice. Inform the MOH MedSafe office of the numbers.
Ceasing to prescribe
Notify the Ministry of Health that you no longer require these pads.
Receipt of excess pads
Notify the Ministry of Health that you no longer require these pads. Destroy or return any unused pads to the Ministry of Health
Suboxone specific issues
Suboxone specific issues
Buprenorphine/Naloxone - Absorption, distribution and half-life
- Buprenorphine/naloxone is a combination of buprenorphine (a semi-synthetic partial opiate agonist) and naloxone (a full opiate antagonist). It is used in opioid substitution treatment as an alternative to methadone.
- Both buprenorphine and naloxone are rapidly metabolized in the small intestine and liver and both have very poor bioavailability when taken this way. For this reason, buprenorphine/naloxone is taken sublingually: buprenorphine has rapid absorption and good bioavailability via this route, whereas bioavailability for sublingual naloxone remains poor. Once absorbed, buprenorphine undergoes rapid distribution and readily crosses the blood-brain barrier. Although the serum half-life of buprenorphine is only around 3 hours, it has a very high affinity for the mu-opioid receptor, and once across the blood-brain barrier it will exert a clinical effect for 24-36 hours.
- The naloxone is to discourage intravenous use. If taken intravenously, naloxone has good bioavailability and exerts a strong antagonist effect at the opioid receptors. This is likely to cause unwanted symptoms of opiate withdrawal in those who are opiate tolerant.
- As a partial opiate agonist, buprenorphine exhibits a plateau effect with increasing dose, and this makes it far safer in overdose than a full agonist such as methadone. As the risk of accumulating a toxic dose is reduced, doses can be increased more frequently during the induction/ titration phase of treatment, and with specialist drug service supervision, daily increases in dose are possible until stability is achieved.
- *See Appendix 3 Pharmacology and Pharmacokinetics of Methadone and Buprenorphine page 97 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
Buprenorphine/Naloxone toxicity
- Buprenorphine is a partial opiate agonist and unlike full agonists (morphine, methadone), the pharmacological effects of buprenorphine exhibit a "ceiling effect" with increasing doses. This makes buprenorphine/naloxone safer in overdose than, say, methadone, as the negative opiate effects (eg respiratory depression) are also constrained by this ceiling effect. Nevertheless, certain groups may be particularly vulnerable to respiratory depression, eg children, those who are opiate-naïve or individuals with chronic obstructive pulmonary disease, and care should be taken to consider these factors when prescribing.
- Although buprenorphine is far safer than full opiate agonists in overdose, there have been some reports of fatalities in adult users, and in particular where there have been contributing factors including:
- Opiate-naïve users.
- Co-use of other substances (alcohol, benzodiazepines).
- Use by crushing and snorting (although this risk is reduced with buprenorphine/naloxone due to the presence of naloxone).
- Children who accidentally ingest buprenorphine/naloxone are particularly at risk of toxic effects:
- Toxic effects are more pronounced in children under 2 years of age.
- In retrospective studies, effects below 2mg dose were unlikely to be severe but at least some effects (lethargy, nausea, vomiting) occurred in all children who ingested 4mg or more.
- Respiratory depression occurred in 7% of paediatric overdoses, and coma in 3%.
- Immediate hospital treatment must be sought in every case where a child or a non-tolerant adult has ingested buprenorphine/naloxone. Similarly, those who are prescribed buprenorphine/naloxonemust be medically assessed if overdose or co-use of other respiratory depressants (alcohol, benzodiazepines) is suspected.
Metabolism and excretion
Buprenorphine is primarily metabolized via the cytochrome P450 pathway in the liver. Care should be taken when co-prescribing medications which induce this pathway (carbamazepine, phenytoin, phenobarbital, rifampin, reverse-transcriptase inhibitors) or inhibit it (azole antifungals, macrolide antibiotics, protease inhibitors). Buprenorphine metabolites are primarily (70%) eliminated in the faeces by biliary excretion, with the remainder excreted in the urine. Naloxone is eliminated via the urine.
Side effects of buprenorphine/naloxone
Very common (reported in at least 10% of patients)
- headache, withdrawal syndrome (usually during induction phase of treatment)
- constipation
- insomnia
- increased perspiration.
Common (reported in at least 1% of patients)
|
§ Chills/ 'flu'-type symptoms |
§ Peripheral oedema |
|
§ Tiredness/ malaise |
§ Parasthesia |
|
§ Reduced appetite/ weight loss |
§ Somnolence |
|
§ Nausea and vomiting |
§ Abnormal liver function |
|
§ Abdominal cramps |
§ Depression/ increased anxiety |
|
§ Diarrhoea |
§ Cough/ pharyngitis/ rhinitis |
|
§ Hypertension |
§ Rash/ pruritus/ urticaria |
|
§ Vasodilation |
§ Lacrimation disorder |
|
§ Reduced libido |
§ Amblyopia |
|
§ Impotence |
§ Irregular menstrual cycles |
|
§ Leg cramps/ myalgia/ back pain/ chest pain/ general pain |
|
|
§ Dental caries |
Many of these symptoms will resolve within a few days of commencing treatment. Other, more long term concerns may be managed by changes in behaviour and lifestyle, eg the increased incidence of dental caries can be managed by improved oral hygiene, dental visits and dietary changes.
*See Section 6.2 Managing Side Effects page 44 and Appendix 4 Side Effects page 101 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
Buprenorphine/Naloxone interactions
Consideration should be given to the potential interactions with Buprenorphine/Naloxone before the following medications are prescribed:
- CNS depressants, narcotics
- general anaesthetics
- mitochondrial toxins (aspirin, isoniazid, valproate, amiodarone, antiviral nucleoside analogues)
- CYP3A4 inhibitors (protease inhibitors, azole antifungals, calcium channel blockers, macrolides)
- CYP3A4 inducers (phenobarbitone, carbamazepine, phenytoin, rifampicin)
- *see Section 4.4 Drug Interactions page 34 and Appendix 5 Drug Interaction page 103 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
The 'precipitated withdrawal' and 'opiate-blocking' effects of Buprenorphine/Naloxone
- The 'precipitated withdrawal' and 'opiate-blocking' effects of buprenorphine/naloxone. Buprenorphine has an extremely high affinity at the mu-opioid receptor but exerts only a moderate effect at the receptor. Consequently, if the initial buprenorphine/naloxone dose is taken too soon after the last use of another opiate, buprenorphine will both displace that opiate and cause a marked reduction in overall opiate effect. This is the so-called 'precipitated withdrawal' effect, which can be both unpleasant and frightening for opiate-dependent patients. Precipitated withdrawal is not reversible once triggered, although the effects will pass within a few hours and symptomatic relief during this time may be useful.
- To avoid precipitated withdrawal, care must be taken to ensure that sufficient time has elapsed since the last opiate dose, usually at least 12-24 hours for a short-acting opioid such as dihydrocodeine. Checking that a patient is in at least mild opiate withdrawal before starting buprenorphine/naloxone, eg by using the Clinical Opioid Withdrawal Scale, can be useful. Transition to buprenorphine/naloxone from longer-acting opioids, eg methadone, requires a much longer abstinence period, and this is best carried out under the supervision of specialist alcohol and drug services. In these situations, a mico-dosing regime could be utilised.
- Once successfully inducted onto buprenorphine/naloxone, the strong affinity of buprenorphine for the mu-receptor means that the consequences of the patient subsequently using unprescribed opiates are unpredictable. Usually, the buprenorphine will prevent the opiate from accessing the receptors and the user will feel that the opiate has had no effect at all - this is the so-called 'blocking effect'. In some cases however, using another opiate may trigger a precipitated withdrawal event. Some patients have been known to try to override the blockade effect of buprenorphine by taking very large doses of opiates; such behaviour is extremely risky in terms of accidental overdose and if such behaviour is suspected treatment should be reviewed, including the suitability of buprenorphine/naloxone as a treatment choice.
Dosing and maintenance treatment
- Initial dose is usually 2-4mg buprenorphine/naloxone on the first day with subsequent doses titrated upwards against withdrawal symptoms in 2-4mg increments, to a maximum daily dose of 32mg. For most patients, good compliance can be achieved in the range 8-16mg daily. Unlike methadone there are no buprenorphine/naloxone 'fast metabolizers' and once-daily dosing is appropriate for the vast majority of patients.
- For some patients who have had a suitable period of stabilisation at a regular daily dose, the frequency of dosing may be reduced to alternate-days at twice the titrated daily dose, with no reduction in clinical effect. For example, a patient stable at 8mg buprenorphine/naloxone daily may be prescribed 16mg on alternate days. However, the maximum dose given on any one day should never exceed 32mg and alternate-day dosing should only be done with the full informed consent of the patient.
Resources
Resources
For providers
- GP Shared Care manual [DOCX, 998 KB]
- GP Shared Care 3 monthly OST patient review checklist [PDF, 88 KB]
- GP Shared Care agreement [PDF, 131 KB]
- Authority for GP to prescribe controlled drugs for the treatment of addiction [PDF, 64 KB]
- NZ practice guidelines for OST [PDF, 1 MB]
- National OST training programme [PDF, 582 KB]
- Best practice article on opioid addiction October 2014 (external link)
- BOP community pharmacy feedback form [PDF, 274 KB]
- Auckland opioid treatment service website and resources (external link)
- Regional Maori health services cultural practice manual [PDF, 439 KB]
For patients
Acknowledgements
Acknowledgements
This pathway was developed in collaboration with:
Service |
Name |
|---|---|
|
Mental Health SMO Tauranga |
Sue Mackersey* |
|
WBOPPHO GP |
Jocelyn Heard* |
|
GP Liaison Nurse - OST |
Andy Walford |
|
WBOPPHO GP |
Tony Farrell |
|
Clinical Team Leader, BOP Addiction Service |
Paula Abbey |
|
Clinical Lead BOPAS |
Sally Whitelaw |
|
Mental Health SMO |
David Chaplow |
|
Community Pharmacist |
Rebecca Lukey |
|
P&F |
Lesley Watkins |
|
Pain Service |
Vicky Beveridge |
|
Program Manager Bay Navigator |
Caroline Davy |
*Pathway lead
Opiod substitution treatment (OST)
Background
Background
About substance abuse and drug dependency
Substance misuse is defined as use of a substance for a purpose not consistent with legal or medical guidelines, the substance having a negative effect on health or functioning and may take the form of drug dependence.
Dependence is defined as:
- a strong desire to take a substance, or difficulty in controlling its use
- the presence of a physiological withdrawal state
- tolerance of the use of the drug
- neglect of alternative pleasures
- persistent use of the drug despite harm to self and others.
Aims of OST
Aims:
- contribute to improving the health of patients as well as aspects of their personal and social functioning
- focus on improvements to quality of life such as education, employment, relationships with significant others
- reduce the spread of infectious diseases associated with injecting drug use, especially hepatitis B and C and HIV/AIDS
- reduce the mortality and morbidity resulting from the misuse of opioid drugs
- assist individuals to achieve successful withdrawal from opioid
- reduce episodes of illegal and other harmful drug use
- reduce crime associated with opioid use.
All aspects of service provision are aimed at reducing harm to the individual, the family/whanau and the community.
The Opioid Substitution Treatment offered should:
- suppress opioid withdrawal and craving
- not induce sedation or euphoria.
Maintenance doses are individualised to assist the patient to achieve their negotiated treatment goals.
Any increase or decrease in dose should be based on a clinical assessment. This clinical assessment might include a serum methadone level.
To achieve these aims the service focuses on:
- delivering person-centred, services that are both accessible and acceptable to patients
- maintaining a partnership approach with patients
- adopting a motivational rather than confrontational approach
- adopting prescribing practices that are evidence and strengths based
- supporting planned withdrawal from methadone or buprenorphine/naloxone when appropriate
Patient confidentiality and privacy are maintained in accordance with relevant legislation and patient consent is obtained in line with the requirements of the Code of Health and Disability Services Consumer Rights Act 1996.
*See Section 1.1 Objectives of OST page 4-5 of " New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
How does OST shared care work?
Why transfer to GP Shared care?
OST aims to support patients to live as normal a lifestyle as possible within the parameters of treatment. GP shared care has the benefits of;
- Instigating more comprehensive health care for patients.
- Allowing services to focus on patients in need for intensive specialist input.
- Improving social integration by normalizing patients treatment.
The phases of treatment provide a patient pathway based on recovery principles. A person may or may not move sequentially through the phases from high intervention to low intervention, but as with any recovery process, may experience periods of higher intervention (re-stabilisation or a return to specialist maintenance) as part of their recovery.
Underpinning the practices and policies of BOPAS is local and international research which demonstrates the effectiveness of Opioid Substitution Treatment (OST). Treatment provided by BOPAS is delivered within a framework of sound medical practice, accepted standards, approved guidelines and legal requirements. BOPAS seek to ensure that methadone or buprenorphine/naloxone is prescribed and dispensed in a clinically responsible manner.
Roles and responsibilities
- The BOPAS lead medical officer as authorising medical officer retains overall responsibility for patients on the GP Shared Care programme.
- GP authorization is based on a shared care model of service delivery. BOPAS provide specialist support and can always be accessed for advice or assistance. Renewal of authorization is contingent upon prescribing practices remaining consistent with BOPAS policy and regular review with lead clinician.
- For roles and responsibilities of the patient, GP and BOPAS, please see documents below:
- Bay of Plenty Addiction service GP Shared Care Agreement (external link).
- Authority for a general practitioner to prescribe controlled drugs for the treatment of addiction (section 24(2) (d) MODA (external link)).
- For information regarding writing of scripts and the storage etc. of script pads please click here. (external link)
See Section 8 OST in Primary Care page 60-62 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
Assessment
Assessment
Instability indicators:
- problematic, harmful or hazardous use of alcohol or other drugs
- engages in or supports criminal activity
- signs of intoxication at clinic or pharmacy
- evidence of intravenous injecting
- irregular dosing
- poor attendance at appointments
- avoidance of urinalysis or blood tests
- behavioural problems such as aggression
- frequently requests changes to dispensing
- requests to replace lost or stolen doses
- any co-existing mental or physical health problems are difficult to treat or are not well managed.
- *see Section 1.2 Roles of Specialists OST Services page 5 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
Stability indicators:
- defined and progressing towards treatment goals.
- no problematic, harmful or hazardous use of alcohol or drugs.
- no evidence of criminal activity.
- responsible management of takeaways.
- schedules and attends appointments.
- rarely requests changes to dispensing.
- social stability as evidenced by relationships with others, stable and healthy housing, employment/occupation.
- any co-existing mental or physical health problems are well managed.
- participates in primary health care.
- complies with programme requirements.
Recommended reviews:
- Appointments:
- Initially the patient will see his/her GP every 28 days when a new script is needed. This is recommended to occur for at least 3 months when the patient is new to your practice. Where there is an established relationship with the patient or there are other indications for less frequent appointments this can be negotiated between the GP, patient and Addiction Liaison Clinician (from the BOPAS service).
- After this initial time the patient must be seen by the GP once every 3 months for a review. The patient usually collects their script from the GP, practice nurse or receptionist at their review and in the two months between the three monthly appointments.
- Three monthly review
- Click here to access the GP Shared Care Patient Review checklist (external link)
- Not attending appointments
- If a patient consistently does not attend appointments, the GP may refrain from writing any further scripts until the patient is seen or may write a short-term interim prescription until a new appointment can be scheduled. The GP should also contact the case manager and or the Addiction Liaison Clinician.
- GP - Six Monthly Information Forms
- The Addiction Liaison Clinician will contact your practice at least every six months to update information. Please provide any additional information you may wish to raise at this time or any time between contacts. It is essential for BOPAS to have current information for continued GP prescribing authorisation.
Management
Management
Visit the drug or drug-related issues pathway (external link) or prescribing issues pathway (external link)
BOPAS Contacts
Bay of Plenty Addiction Service (BOPAS)
Postal address:
Kowhai House
Tauranga Hospital
Cameron Road
Private Bag 12024
Tauranga 3143
Opening hours: Monday to Friday, 8.30am to 5pm
- email: bopas@bopdhb.govt.nz
- phone reception: 07 579 8391
- phone crisis team (after hours): 07 579 8329 or 0800 800 508
Concurrent issues
Pain Management
Acute pain:
- Mild to moderate acute pain can usually be effectively managed with simple analgesics (including mild opioid medications) and/or other appropriate medications.
- Opioid maintenance patients with acute severe pain usually require higher doses of opioid agonists than non-opioid tolerant patients in order to achieve adequate pain relief. (Many receive inadequate analgesia for acute severe pain).
- In the event an OST patient is hospitalised their GP prescriber will need to liaise with the hospital staff to ensure continuation of methadone or buprenorphine/naloxone in hospital, cancellation of the prescription at the community pharmacy and the resumption of prescribing at the community pharmacy on discharge. BOPAS can assist as required.
Chronic pain:
- Chronic pain in Opioid maintenance patients should be managed in the same way as it is for other patients.
- Methadone or buprenorphine/naloxone as prescribed for maintenance treatment may provide partial relief for some chronic pain.
- BOPAS advises consultation with a specialist pain management service or BOPAS medical officer before considering the regular prescribing of opioid medication for the management of chronic pain.
- Note: Long term methadone treatment can saturate and dull opioid receptors leading to increased patient pain levels as the body tries to compensate for inhibited pain recognition (hyper-analgesia; increased sensitivity to pain secondary to long-term blockade of opiate-based pain receptors)
- *See Section 6.6; 6.6.1; 6.6.2 Management of Acute and Chronic Pain page 49 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
Pregnancy:
- There are several health problems during pregnancy that should be discussed including:
- General nutrition.
- Risks of anaemia.
- Alcohol and nicotine consumption.
- Oral hygiene and dental health.
- Complications from chronic infection related to injection practice.
- Antenatal and postnatal mental health problems.
- Advice should be given regarding potential complications of pregnancy associated with drug use:
- Premature delivery.
- Low birth weight.
- Placental abruption.
- Neonatal abstinence syndrome.
- Opioid detoxification in pregnant women:
- Should be undertaken with caution; and
- In the second trimester with small frequent reductions − however, expert opinion suggests that a patient should be free to choose to initiate detoxification at any stage of pregnancy, provided her circumstances and her ability to cope are taken into consideration.
- Partial splitting of the dose may also be considered for stable pregnant patients in the latter half of pregnancy in order to avoid the necessity for increase in the dose, especially for those on doses below 60mg. A single daily dose should be reinstituted following delivery.
- Note: A small number of women become fast metabolizers of methadone or buprenorphine/naloxone in pregnancy. Where this is suspected, obtain trough and peak serum methadone levels and discuss with the BOPAS before instituting split dosing. These women are at greater risk of destabilization in pregnancy and timely assessment and management can prevent this.
Breastfeeding:
- In general, it is safe to breastfeed while a mother is taking methadone as long as there are no other factors that would make breastfeeding unsafe, such as using illegal drugs or using certain prescription medications. Methadone is found in breast milk, but only a small amount gets passed along to the baby.
- There are many benefits to breastfeeding for both the mother and her baby including:
- Breast milk has important nutrients that will help baby grow and may help prevent infection.
- Babies who are breastfed are generally more healthy and don't have to visit the doctor as often as babies who are fed formula.
- Breastfeeding helps the mother and her baby bond.
- Breastfeeding may help baby cope with withdrawal symptoms.
- Although there is no official statement saying that mothers cannot breastfeed if they are taking methadone, it would be wise to discuss this with the specialist service to learn more about it.
- *See Section 6.7 Management of Pregnant and Breastfeeding Women page 52-56 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
Concurrent Medical Conditions
HIV/hepatitis B and C
- Issues for the GP managing a patient on Opioid Substitution Treatment (OST) are:
- testing for HIV, Hepatitis A, B and C (including Hep C PCR RNA test)
- preventing infection/transmission
- monitoring LFTs in those with chronic Hepatitis B and C
- offering treatment for hep C, or refer for specialist treatment where required
- offering Hepatitis A and B vaccination to those who are HAV and HBV antibody negative.
Chronic liver disease
- Patients with chronic liver disease on long-term opioid maintenance usually do not require alterations in their dose. However, if there is an abrupt change in liver function they may require dose adjustment. The development of jaundice is also a sign that the liver may not be able to metabolize methadone or buprenorphine/naloxone at the normal rate.
- Where there is significant impairment it is suggested that the methadone serum level is checked every 2 to 3 months to ensure that it is not rising due to impaired metabolism of methadone. Seek the advice of BOPAS or a specialist gastroenterologist if there are concerns.
Respiratory disorders
Methadone or buprenorphine/naloxone is a respiratory depressant and care should be taken in prescribing methadone or buprenorphine/naloxone to patients with these disorders.
Epilepsy
Note that carbamazepine, phenytoin and phenobarbitone interact with methadone (see methadone or buprenorphine/naloxone interactions section).
Mental health disorders
Note that antidepressant and antipsychotic medications may interact with methadone or buprenorphine/naloxone (see methadone or buprenorphine/naloxone interactions).
Resources
Resources
For providers
- GP Shared Care manual [DOCX, 998 KB]
- GP Shared Care 3 monthly OST patient review checklist [PDF, 88 KB]
- GP Shared Care agreement [PDF, 131 KB]
- Authority for GP to prescribe controlled drugs for the treatment of addiction [PDF, 64 KB]
- NZ practice guidelines for Opioid Substitution Treatment [PDF, 1 MB]
- National Opioid Substitution Treatment Training Programme [PDF, 582 KB]
- Best practice article on Opioid Addiction October 2014 (external link)
- BOP community pharmacy feedback form [PDF, 274 KB]
- Auckland opioid treatment service website and resources (external link)
- Regional Maori health services cultural practice manual [PDF, 439 KB]
For patients
- OST and you - A guide to Opioid Substitution Treatment
About the Tauranga Opioid Substitution Treatment service (OST)
The Tauranga Opioid Substitution Treatment service (OST) is one of the services offered by Bay of Plenty Addiction Service (BOPAS) that is part of Mental Health and Addiction Services, Bay of Plenty District Health Board (BOPDHB).
This pathway contains information and guidelines for General Practitioners authorized by BOPAS OST to prescribe methadone or buprenorphine/naloxone to patients in the GP Shared Care Programme. BOPAS OST intends that this information will assist in the provision of a quality, safe, professionally delivered OST Service that meets the needs of patients, their family/whanau, and the wider community. GPs and their staff are encouraged to consult with the Addiction Liaison Clinician or the Lead Clinician at BOPAS OST working in a shared-care partnership model.
BOPAS OST provides services for the management of opioid dependency from a harm reduction philosophy, supporting people towards recovery, relative to each individual and his or her own circumstances.
The OST programme is in accordance with:
The BOPAS Service manages the admission, stabilisation and specialist maintenance phases of OST treatment. Patients may then be assessed as meeting criteria for the GP Shared Care Programme where their OST is integrated with their primary health care provider who is authorised by BOPAS on a three-monthly (6-monthly with permission from the MOH) basis to prescribe methadone or buprenorphine/naloxone.
Acknowledgements
Acknowledgements
This pathway was developed in collaboration with:
Service |
Name |
|---|---|
|
Mental Health SMO Tauranga |
Sue Mackersey* |
|
WBOPPHO GP |
Jocelyn Heard* |
|
GP Liaison Nurse - OST |
Andy Walford |
|
WBOPPHO GP |
Tony Farrell |
|
Clinical Team Leader, BOP Addiction Service |
Paula Abbey |
|
Clinical Lead BOPAS |
Sally Whitelaw |
|
Mental Health SMO |
David Chaplow |
|
Community Pharmacist |
Rebecca Lukey |
|
P&F |
Lesley Watkins |
|
Pain Service |
Vicky Beveridge |
|
Program Manager Bay Navigator |
Caroline Davy |
*Pathway lead
OST prescribing issues
Background
Background
About opioid substitution treatment prescribing issues
The Tauranga Opioid Substitution Treatment service (OST) is one of the services offered by Bay of Plenty Addiction Service (BOPAS) that is part of the wider Mental Health and Addiction Services at Health New Zealand Bay of Plenty.
This pathway contains information and guidelines for general practitioners authorized by BOPAS OST to prescribe methadone or buprenorphine/naloxone to patients in the GP Shared Care Programme. BOPAS OST intends that this information will assist in the provision of a quality, safe, professionally delivered OST Service that meets the needs of patients, their family/whanau, and the wider community. GPs and their staff are encouraged to consult with the Addiction Liaison Clinician or the Lead Clinician at BOPAS OST working in a shared-care partnership model.
BOPAS OST provides services for the management of opioid dependency from a harm reduction philosophy, supporting people towards recovery, relative to each individual and his or her own circumstances.
The OST programme is in accordance with:
The BOPAS Service manages the admission, stabilisation and specialist maintenance phases of OST treatment. Patients may then be assessed as meeting criteria for the GP Shared Care Programme where their OST is integrated with their primary health care provider who is authorised by BOPAS on a three-monthly (6-monthly with permission from the MOH) basis to prescribe methadone or buprenorphine/naloxone.
Prescribing issues
Prescribing issues
-
What to do when GP on leave or absent
- GPs are urged to appoint a locum or practice partner to prescribe methadone or buprenorphine/naloxone to their authorised patients in their absence and to ensure that BOPAS, locum/practice partner and other practice staff are informed of this.
- The BOPAS OST, Addiction Liaison Clinician is also available to support the locum/practice partner.
- Should the GP plan to be away for longer than three months he/she needs to contact the Addiction Liaison Clinician so that BOPAS OST service can arrange authorization(s) for the locum or a practice partner (as required by Medsafe) and provide training and extra support.
-
Prescribing for holidays or travel
- Public holidays (Please contact BOPAS for support as required):
- The GP is responsible for identifying when a patient's dispensing day/s fall on a public holiday and should annotate the prescription accordingly, i.e., write instructions for any change in dispensing required due to closure of the pharmacy. If space is limited use an additional sheet and attach it to the prescription. The Addiction Liaison Clinician can assist with a generic holiday schedule that can be adjusted to suit individual needs.
- It is preferred that no more than three consecutive takeaway doses are approved at any one time, except in the case of public holidays where pharmacies are not providing a service or in exceptional circumstances. In such cases 1 (one) additional takeaway dose (i.e., a total of four takeaway doses) may be prescribed for a patient providing the Patient, the Addiction Liaison Clinician and the GP are confident that it is a safe arrangement.
- Patient holidays (within New Zealand):
- The GP, with Addiction Liaison Clinician support, is responsible for organising alternative dispensing arrangements for patients on holiday. See transfers between pharmacies.
- Patients should provide the GP with adequate notice of holidays.
- Travel overseas:
- GPs are advised to contact the Addiction Liaison Clinician for information and assistance with arranging overseas travel as soon as they receive a request from a patient. It is preferred that arrangements be made for the patient to be dispensed methadone or buprenorphine/naloxone via a programme in the country of destination.
- Note: If the patient needs to travel with methadone or buprenorphine/naloxone doses they will require an exportation letter (explains dose and form (usually tablets) prescribed and the dates the medication is prescribed for).
- Adequate notice (usually several weeks) is required to make these arrangements. More time may be required when a patient is travelling to more than one destination or where other complexities exist. There are a number of countries where OST is not available and/or where importation of methadone or buprenorphine/naloxone is illegal. In an emergency situation overseas travel may be arranged more quickly but this does not apply to all countries of destination.
- *See Section 5.7 Travelling Overseas with Opioid Substitution Medication page 40 of “New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
- Public holidays (Please contact BOPAS for support as required):
-
Take away arrangements
- Methadone or buprenorphine/naloxone Takeaway Arrangements:
- A takeaway dose of methadone or buprenorphine/naloxone is any dose that is not consumed under observation at the dispensing pharmacy.
- Takeaway arrangements in the GP Programme continue to be based on clinical safety and within the National Practice Guidelines.
- Note: The National Practice Guidelines recommend that methadone or buprenorphine/naloxone should be observed to be consumed at the pharmacy or other dispensary on at least three non-consecutive days per week.
- Variance: Where the authorised GP and the patient assess that less frequent dispensing is appropriate, this is notified to Addiction Liaison Clinician for BOPAS OST team review. Once the OST service supports the requested change, a new authorisation would need to be prepared to reflect these changes. A copy will be sent to the GP, the pharmacy and the Ministry of Health.
- Following the review any variance from the above policy needs to be documented and referenced in relation to the indicators of stability and instability. Evidence such as proof of employment might be required to support requests for less frequent observation.
- Note:
- Every client in New Zealand must consume observed at least once weekly.
- GPs are advised to refrain from making any changes to takeaway arrangements during the first 3 to 6 months in the GP programme to enable time to fully assess the patient and their safety with further takeaways.
- *See Section 5.1 Takeaway Doses page 36 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
- Methadone or buprenorphine/naloxone Takeaway Arrangements:
-
Requests for replacement doses
- Replacement Doses: BOPAS OST policy is not to replace doses under any circumstances e.g., lost, stolen, spilt, damaged, retched.
- If in exceptional circumstances that can be verified (i.e., by a police report, eyewitness by professional), the GP may (after discussion with the BOPAS OST service) offer to assess the patient 48 hours or more after their last dose was consumed and if there are signs of opioid withdrawal then part of subsequent doses may be replaced. When requests are made for replacement doses the GP should review the person's takeaway arrangements and notify the case manager and or Addiction Liaison Clinician.
- BOPAS policy is to replace 50% of a vomited methadone dose when the patient vomits within approximately 30 minutes of consuming the dose, the vomiting was witnessed by a professional and the replacement is clinically appropriate. (e.g., pregnancy)
- As buprenorphine/naloxone is absorbed sublingually, there is no need to replace doses after vomiting.
- If a second replacement dose for vomiting is requested within a short time, or there are regular requests for replacement doses, no further replacement doses should be authorized until the patient has been assessed by the GP and any underlying cause for the vomiting assessed and treated.
- All replacement doses must be prescribed on a new H572M prescription and must be consumed in the pharmacy.
- Note: repeatedly seeking replacement dose is likely instability indicator.
- *See Section 5.3; 5.3.1; 5.3.2 Replacement Doses page 38 of “New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
-
Agents acting on behalf
- Agents Collecting on Behalf of a Patient: A GP can authorise an agent to collect OST on behalf of a patient in extraordinary circumstances where the patient is unable to attend the pharmacy e.g., when they are house-bound due to illness. Circumstances necessitating the authorization of an agent must be verified with the patient and the agent.
- Authorization of an agent is limited to a maximum of 3 doses of methadone or buprenorphine/naloxone dispensing.
- Authorization must be made in writing and faxed to the appropriate pharmacy and include:
- Name and address of the agent.
- Type of identification provided by agent.
- Number of doses the agent is authorised to collect.
- Signature of the authorising GP
- The authorised agent must provide suitable identification.
- Note: The GP must feel confident that the authorised agents can responsibly manage and administer the methadone/ buprenorphine/naloxone.
- Discussion about safety of takeaways is essential e.g., storage away from children, no replacement of lost or stolen doses.
-
How to write a prescription
- Writing a methadone H572 controlled drug prescription
- The use of H572M controlled drug prescription forms is restricted to prescribing methadone for patients under the authority conferred by Section 24(2) (d) Misuse of Drugs Act 1975 (i.e., where BOPAS has authorised a prescriber for a specific patient). The form is not used for prescribing of methadone to other patients in other circumstances (e.g., pain relief for a non-BOPAS client); in these cases, the general H572 controlled drug prescription is used.
- H572 Prescription example and instructions (external link)
- Ordering
- These CD pads are requested 3-6 monthly by GPs based on their current number of authorised patients.
- Orders are faxed to the Ministry of Health using the approved order form (refer to Forms section). On receipt of the pads, sign the enclosed verification of delivery form and fax to the Ministry of Health as soon as possible.
- Ministry of Health contacts
- MedSafe Office - ph. 09 441-3670
- Storage
- These CD pads must be stored in a secure place as for other CD prescription pads. You are advised to keep the receipt for the pads as a record of the prescription pad numbers.
- Theft of prescription forms
- If the prescription numbers are known, inform the Ministry of Health MedSafe office. If the prescription numbers are unknown, inform the Ministry of Health and request the prescription numbers of the pads recently sent to the practice. Inform the MOH MedSafe office of the numbers.
- Ceasing to prescribe
- Notify the Ministry of Health that you no longer require these pads.
- Receipt of excess pads
- Notify the Ministry of Health that you no longer require these pads. Destroy or return any unused pads to the Ministry of Health
- Writing a methadone H572 controlled drug prescription
-
Split Methadone or Buprenorphine/Naloxone dosing
- For the vast majority of patients adequate stability can be achieved on a once daily dose of methadone or buprenorphine/naloxone.
- Patients in GP shared care are unlikely to require a change to split dosing, unless in exceptional circumstances.
- Partial splitting of the dose may also be considered for stable pregnant patients in the latter half of pregnancy in order to avoid the necessity for increase in the dose, especially for those on doses below 60mg. A single daily dose should be reinstituted following delivery--See OST and Pregnancy (external link)
- Note: A small number of women become fast metabolizers of methadone or buprenorphine/naloxone in pregnancy. Where this is suspected, obtain trough and peak serum levels and discuss with the BOPAS before instituting split dosing. These women are at greater risk of destabilization in pregnancy and timely assessment and management can prevent this.
- Split dosing may also be considered for stable patients in the latter part of a planned withdrawal from methadone or buprenorphine/naloxone (usually at doses of 30mg or less) in order to reduce pre-dose withdrawal symptoms and to increase the likelihood of successful completion of withdrawal from methadone or buprenorphine/naloxone. This needs discussion with and authorisation by the OST service.
- Split dosing may be in exceptional circumstances considered for stable patients to better manage physical pain symptoms.
- Split dosing(including the proportions of each dose) requires the approval of the BOPAS
- *See Section 5.6 Split Methadone Doses page 40 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
-
Transfers between pharmacies
- The case manager and or addiction liaison clinician may assist you with this.
- Otherwise:
- Establish with the patient which dispensing pharmacy in the area is suitable and confirm with the pharmacy that they are able to dispense to the patient.
- Cancel the script at their existing pharmacy.
- Write a new script for the new pharmacy and fax it to them if necessary.
- Contact the Addiction Liaison Clinician to request that an 'Introduction to Pharmacy' letter with a photo ID is sent to the new pharmacy.
- The patient will be required to provide photo-ID at the new pharmacy.
-
Transfer to another OST Programme
- Contact the BOPAS OST with details about the proposed new location of the patient and request assistance with the transfer.
- Note: Waiting times for transfer to other OST programmes vary considerably throughout the country.
- Where a patient is stable the treatment service at the new location may agree to the transfer of the patient directly to a GP authorised by that service and the transfer may be achieved more quickly. Alternatively, out of area prescribing may be arranged until such time as the local OST service is able to take them onto their programme. However, during this interim period the patient should return to be seen at least 3 monthly by their prescribing doctor. The Specialist OST service will not be able to authorise an out of area GP.
- *See Section 7.1 Transferring between Specialist Services page 57 of "New Zealand Practice Guidelines for Opioid Substitution Treatment 2014 (external link)"
-
Managing missed doses
- The pharmacy should notify you if the patient misses any doses. Three or more consecutive missed doses as under National protocols the patient must be reassessed by the BOPAS OST service, before dispensing can resume. They need to be seen and assessed as to whether it is safe for them to resume dispensing the usual dose or whether they require a dose decrease due to reduced tolerance. Opioid tolerance rapidly changes, so several days without opioids can significantly alter tolerance to prescribed OST.
Resources
Resources
For providers
- GP Shared Care manual [DOCX, 998 KB]
- GP Shared Care 3 monthly OST patient review checklist [PDF, 88 KB]
- GP Shared Care agreement [PDF, 131 KB]
- Authority for GP to prescribe controlled drugs for the treatment of addiction [PDF, 64 KB]
- NZ practice guidelines for OST [PDF, 1 MB]
- National OST training programme [PDF, 582 KB]
- Best practice article on opioid addiction October 2014 (external link)
- BOP community pharmacy feedback form [PDF, 274 KB]
- Auckland opioid treatment service website and resources (external link)
- Regional Maori health services cultural practice manual [PDF, 439 KB]
For patients
Acknowledgments
Acknowledgments
This pathway was developed in collaboration with:
Service |
Name |
|---|---|
|
Mental Health SMO Tauranga |
Sue Mackersey* |
|
WBOPPHO GP |
Jocelyn Heard* |
|
GP Liaison Nurse - OST |
Andy Walford |
|
WBOPPHO GP |
Tony Farrell |
|
Clinical Team Leader, BOP Addiction Service |
Paula Abbey |
|
Clinical Lead BOPAS |
Sally Whitelaw |
|
Mental Health SMO |
David Chaplow |
|
Community Pharmacist |
Rebecca Lukey |
|
P&F |
Lesley Watkins |
|
Pain Service |
Vicky Beveridge |
|
Program Manager Bay Navigator |
Caroline Davy |
*Pathway lead